Depression Is Bad
Is depression as bad as people think? The short answer is, YES it is!
Yes depression is as bad as people think. However, it is a complicated issue and generally misunderstood.
Clinical depression or Major Depressive Disorder (as defined by the Diagnostic and Statistical Manual of Mental Disorders-5th edition: DSM-V) is very serious.
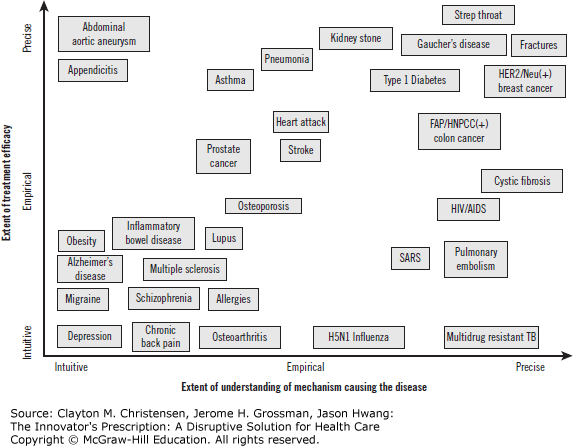
The reality we must face, however, is that diagnosis is intuitive rather than precise.
Many people will be labeled “depressed”, or will label themselves depressed, when in fact they are experience a normal range of human emotions. Affect within normal range (ie..you are sad because you should be sad).
Manual of Mental Disorders: DSM-5
The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition: DSM-5 outlines the following criterion to make a diagnosis of depression.
The individual must be experiencing five or more symptoms during the same 2-week period and at least one of the symptoms should be either – (1) depressed mood or (2) loss of interest or pleasure.
- Depressed mood most of the day, nearly every day.
- Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day.
- Significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day.
- A slowing down of thought and a reduction of physical movement (observable by others, not merely subjective feelings of restlessness or being slowed down).
- Fatigue or loss of energy nearly every day.
- Feelings of worthlessness or excessive or inappropriate guilt nearly every day.
- Diminished ability to think or concentrate, or indecisiveness, nearly every day.
- Recurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
Distress or Impairment
To receive a diagnosis of depression, these symptoms must cause the individual clinically significant distress or impairment in social, occupational, or other important areas of functioning.
The symptoms must also. “not be a result of substance abuse or another medical condition”. (from PsyCom: Depression Definition and DSM-5 Diagnostic Criteria)
There are other conditions which reach clinically significant levels.
The most common being Persistent Depressive Disorder (used to be called Dysthymia). The condition is not as “deep” or “severe” as MDD. However, PDD has its own unique set of challenges.
Criteria From The DSM-V:
A. Depressed mood for most of the day, for more days than not, as indicated by either subjective account or observation by others, for at least 2 years. Note: In children and adolescents, mood can be irritable and duration must be at least 1 year.
B. Presence, while depressed, of two (or more) of the following:
- Poor appetite or overeating
- 2. Insomnia or hypersomnia
- 3. Low energy or fatigue
- 4. Low self-esteem
- 5. Poor concentration or difficulty making decisions
- 6. Feelings of hopelessness.
C. During the 2-year period (1 year for children or adolescents) of the disturbance, the individual has never been without the symptoms in Criteria A and B for more than 2 months at a time.
D. Criteria for a major depressive disorder may be continuously present for 2 years.
E. There has never been a manic episode or a hypomanic episode, and criteria have never been met for cyclothymic disorder.
F. The disturbance is not better explained by a persistent schizoaffective disorder, schizophrenia, delusional disorder, or other specified or unspecified schizophrenia spectrum and other psychotic disorder.
G. The symptoms are not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hypothyroidism).
H. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Note: Because the criteria for a major depressive episode include four symptoms that are absent from the symptom list for persistent depressive disorder (dysthymia), a very limited number of individuals will have depressive symptoms that have persisted longer than 2 years but will not meet criteria for persistent depressive disorder.
Treatment Is Required
If full criteria for a major depressive episode have been met at some point during the current episode of illness, they should be given a diagnosis of major depressive disorder. Otherwise, a diagnosis of other specified depressive disorder or unspecified depressive disorder is warranted
Depression, when at the clinically significant/diagnostic level, is “that bad”.
It impacts people on a biological, psychological, and behavioral level.
Treatment of depression requires psychiatric support and talk therapy.
Medicine is available that can help. People should seek professional support as soon as possible.
However sadness is part of life, and the sooner we “jump on” the negative feelings the easier the fix. We need to be careful to not characterize all “low moods” as depression.
Therapist For 15 Plus Yrs
I have been in practice as therapist for 15 plus years. So clearly, I believe in therapy and I believe that depression is real.
As I said above, it is serious and it requires professional intervention and support. But people can also improve their lives without a therapist and feeling down does not automatically equal depression.
People have always struggled with emotional issues and mental health. This is not a modern phenomenon. It’s well documented.
Anxiety, depression, substance misuse have been part of the human condition across history. People found a way through.
Seeking the perfect therapist, or the perfect “program” or
perfect treatment center or perfect combination of medication is an exercise in
frustration. Don’t wait for that perfect solution.
Warning!!!
Stay away from incompetent therapists and providers that suck.
There are a fair number out there. But otherwise, accept support and try to take action.
The action does not have to be perfect and you won’t immediately solve the problem. The “action” can be as simple as evaluating your current behavior in an honest and open manner.
Talk to someone about your struggle. But do so with full investment and vulnerability. Get more information on depression. Try on different ideas.
Maintain Perspective
Bearing the emotional pain of a seriously troubling
circumstance can be “depressing”. This state may not be representative of
depression in the diagnostic or clinical sense. However, it could be the
catalyst for clinical depression.
Address this before it transitions to more serious stage.
Some Suggestions:
A) Get moving (or keep moving). Imperfectly execute on your life and responsibilities. Seek out the presence of other Homo sapiens. Preferably nice ones… with pleasant demeanor and positive attitudes.
B) Perspective taking. Write in your journal. Journal and write about a major difficulty/problem you have gone through in the past where the long term impact/result was not as bad as you anticipated (ie…it all worked out in the end) Write about the outcomes and how it worked out and how you made it through.
C) Engage the free three: 1) listen to upbeat music, 2) laugh, 3) go outside.
D) Identify your preferred thinking error. Mine is catastrophizing. Be on the look out for those type of thoughts (call them ants). Know the ants are coming. Act swiftly and decisively to crush these ants.
E) Have a “go to person”. One on one to talk it out. Obviously a therapist is one option. Also coach, mentor, appropriate family/friends.
F) Tell yourself: “It is possible that I will feel better in the future”… “It is possible that I can be happy again”… etc.
It is important to focus on light at the end of the tunnel. All things pass and if you can hold on you will likely feel better. Watch this video.
Final Words
No matter what. Try to keep moving.
If you aren’t “feeling it” do it anyway.
Make yourself do life in an imperfect manner.
Go through the motions. Show up.
Thanks, Rich Jones