I don’t celebrate Biden’s “addiction funding”if it’s focused solely on your standard systemic model. Based on the typical paradigm.
And, I think this goes way beyond “harm reduction dollars”.
Could we force a fundamental shift in funding and approach. Even if it was on a small scale. From “individual focus” to “family focus”
The Family “Unit”
The “unit” to be reimbursed should be the family as a whole. Not the individual. That would get me fired up.
Let’s think about it.
The “overdose epidemic”, alcohol, suicide. What have become known as deaths of despair.
This reality confronts the theory that underlies our systemic response.
Typical Response
✅ We wait for a client to engage in a specific modality of treatment once they experience a sufficient amount of suffering to become properly motivated.
Also the default, far too often, is to tell the family to stay out of it.
✅ In any given circumstance, the typical response of rehab to meetings to long term recovery may be appropriate. And I am very grateful when that happens.
And, perhaps, there are cases where the family should stay out of it.
But the reality is ….
We can’t wait for motivation produced by suffering. We can’t wait for bottom.
The Long Haul
✅ OVER THE LONG HAUL, family members become continuing care coordinators.
Once the patient leaves rehab it’s back onto the family. They will be responsible for intervening and responding.
I guess some of us are equipped to do that. Strangely enough.
But for the most part, family members are searching in the dark without a flashlight.
Train & Educate The Family
✅ Therefore, we should train and educate the family to intervene. This is just as important as detachment.
Families must become subject matter experts and system navigators.
✅ Better yet, every single family should have a case coordinator that actively engages for at least 5 years.
Qualified Family Recovery Coach
A specially trained and qualified family coach. Regardless of the status of the patient.
Paid for by insurance, Medicaid/Medicare and the state drug and alcohol authorities.
💥💥💥THE FAMILY SHOULD BE THE IDENTIFIED PATIENT(S). NOT THE INDIVIDUAL. 💥💥💥
THAT WOULD PRODUCE CHANGE.
Age of Despair
✅ There is theory … and then there is reality. In the substance use disorder world.
The 2 things don’t match. Not anymore.
Not in the day and age of fentanyl, fake pills, tainted meth and cocaine….
🙏 Not in this age of despair.
The Truth
It’s just the truth. And everyone knows it’s the truth.
Even the people who publicly disagree with me, privately know it’s the truth.
We are plugging holes. Plugging leaks in the sailboat.
We are sinking.
Will you stick around to see us go down?
Courage
Who has the courage to flip the script? Which of the payers will step out and change this tragic predicament overnight?
I feel compelled to respond on some level. And then I will let this go.
Okay… Here we go.
There are a couple of assumptions that are necessary up front. If we are going to have a reasonable conversation about this.
Assumptions
There is such a thing as – SCIENCE.
Research methods apply to social issues. As a society we should be making our decisions and forming our policies based on research. NOT based on my personal (or your personal) experience, strength and hope.
Having a “problem” with drugs and/or alcohol is a – BAD THING.
Regardless of what you call it (addiction, SUD, etc…) it is BAD for your health and bad for society.
Resolving a “problem” with drugs and/or alcohol is a – GOOD THING.
Regardless of what you call it (recovery, remission, getting better etc…). It is good for your health and good for society for the problem to be resolved.
If you can’t agree with these 3 points. There is nothing anyone can say to you to facilitate a meaningful conversation.
You are dogmatically entrenched and an extremist. I wish you the best. I apologize if my opinions offend you.
The Research & Facts
Let me break down the data below. WARNING: This is research. Not opinion:
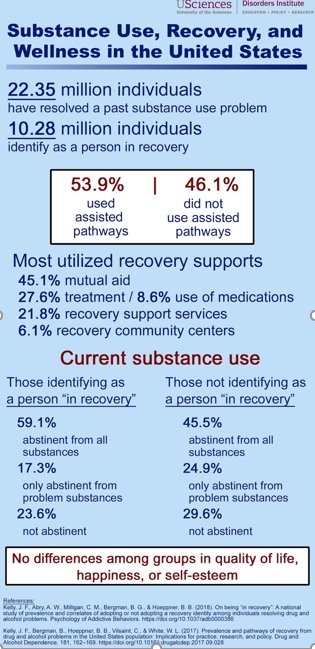
22.35 Million People Have Resolved a Substance Use Problem (over their lifetime). They HAD A PROBLEM. They NO LONGER HAVE A PROBLEM. That is a good thing.
Only 10.28 million call it recovery.
The other 12.07 million just got better. They don’t care if you think it’s recovery. They got better. And that is a good thing.
Of the 22.35 million who got better:
12.04 million (53.9%) got help/assistance.
10.31 million (46.1%) DID IT ON THEIR OWN. They got better (that’s a good thing). And they did it on their own.
Of the 12.04 million who got help:
5.4 million used 12-step meetings or some other type of mutual support group.
3.3 million got treatment and of those 283,800 used medication assisted pathway.
2.6 million were involved with recovery support services.
734,000 were involved with recovery centers.
Therefore, the typical/traditional pathway of meetings and/or treatment accounts for only 8.7 million (5.4 million meetings + 3.3 million treatment) of the 22.35 million who got better.
That’s 39% of the people. It’s an important part of the equation.
BUT THE “TRADITIONAL PATHWAYS” do not account for the majority of change.
61% DID IT SOME OTHER WAY
This should promote dialogue around alternative therapies and new ideas.
Furthermore, if you look a little deeper:
Of the 10.28 who say they are in recovery: **59.1 % report total abstinence. That means 40.9% or 4.2 million moderate.
Of the people who DID NOT say they were in recovery: **45.5% report total abstinence.
That means 55.5% or 6.7 million people moderate.
This leaves us with 10.9 million people who have resolved a problem with substance use via moderation.
That is 48.7%. Nearly half. Nearly half use moderation.
ALSO. THE RESEARCHERS FOUND NO DIFFERENCE IN HAPPINESS LEVELS OR SOCIAL FUNCTIONING AMONG THE GROUPS.
Moderation and total abstinence produced the same quality of life outcomes.
Now at this point. You are left with only a few choices.
Research in general is not real. There is no such thing as science. Therefore, you disregard this information.
This particular research is not real. It was put together by Harvard Medical School and a bunch of idiots “up there”. You are much smarter and much more informed than any of those idiots from Harvard. Therefore, you disregard this information.
You “don’t give a shit about no research”. You know what worked for you and you know what worked for your group and therefore you don’t need no research. You and your 10 or 100 or 1000 acquaintances in recovery speak for all of humanity. All 7.5 Billion people. In which case, you disregard this information.
Or… perhaps there is legitimacy to this research. AND further discussion and exploration is needed.
Certainly, we should be trying to reach people via different avenues. Especially when, it is obvious that multiple pathways (including moderation) work.
Recovery Answers – National Recovery Study – Dr. John Kelly – Multiple Pathways to Recovery Conference
Access the original National Recovery Study research article:
We have been fooled into thinking there are “approved” ways to get better. Approved “Pathways to Recovery”.
When I started my recovery journey 22 years ago it was made clear to me: there is only one way to recover and that is adherence to a prescribed 12-step program.
Specifically, find a sponsor, follow his directions, don’t question his authority, “work” the steps and you will be good to go.
Otherwise, you are screwed. If you deviate from that path you will most certainly “get high” and ultimately die.
The Message
You may think I am exaggerating for effect.
I am not. That was “the message”. And any variation from that “message” was false and dangerous.
Of course, not all members of 12-step communities operated with such intensity. There was a spectrum of “hardass-ness” with the recovery community.
Some people were more reasonable than others. Some people were open-minded and worked collaboratively with their “sponsees”. Although they were labeled “easier and softer” and marginalized within many groups.
Prevailing Attitude
All that aside. The prevailing attitude was “stay on our path” It’s the only legitimate way to recovery.
Fast forward 22 years. Today we say “multiple pathways of recovery”.
It’s become the preferred lingo of the recovery community.
One Size Fits All
This is certainly a better arrangement than one size fits all.
However, the implications are still limited and this phrase does not capture the reality of a journey toward wellness.
What about the famously used – “MULTIPLE PATHWAYS OF RECOVERY” – This terminology can be misleading.
Does this mean we have to “pick a program” and follow that pathway only?
Pick Your Pathways to Recovery
Is there a correct way to “do the program”?
As if there is a menu of approved pathways:12-step, clinical support, favor all recovery, coaching, individual therapy, SMART recovery, and on and on.
Pick one. And do it right.
I would argue, subconsciously, that’s the message many of us receive.
“Reality Check”
Some people pick a path. And that’s all there is to it. Now and forever.
They are on the path. That’s fantastic. Wonderful. However, many of us pick multiple paths.
Even better, many of us take a route that is not defined as a specific pathway or program. The truth is most people figure out their own pathway over time.
With a formal program or without a formal program.
The elements of recovery are many and they are not uniform.
The elements of recovery go way beyond any particular meeting or book or manual.
Recovery is not static. Recovery is fluid and ever-changing. We never “arrive”.
We adjust. We try different things. Things that “worked” stop working.
We do this course correction over and over throughout our recovery.
For the Record
For the record, when I say recovery. I mean “recovery from all matters of the mind”.
Trauma, substance use, mental health struggles, emotional struggles.
“Getting better” in these areas involves a similar journey. I don’t put substance use disorders in a silo.
The most important thing is to keep moving forward.
I have been a therapist for 20 years and several things are obvious.
There is no one way to get better.
There is only “momentum”. We are moving forward, or we a moving backward.
Momentum and progress are many times, imperceptible processes. You can not “see the progress”.
Look for the forward momentum.
And if you are trying to better yourself.
I celebrate you and admire you.
Regardless of the pathway, program or “plan”.
ONE MORE THING, BEWARE THE ABSTINENCE VIOLATION EFFECT
People get really down on themselves for “slips” or mistakes or not following the plan perfectly.
When we make a mistake. We beat ourselves up. We tell ourselves lies:
“Man you suck”… or “Why can’t you get this right”… or “You will never get better”…
Unfortunately, some people will reinforce this negative self-talk.
Even professionals will punish a mistake. This is terrible, but we can tackle that at another time.
FOR NOW PLEASE EMBRACE THE FACTS OF RECOVERY:
We all struggle. We all slip up. In some way or in some form. We are all a work in progress.
A Fully funded, fully independent, fully kick-ass Federal Department of Recovery.
I don’t know why I can’t just chill and wait for the epidemic to “burn itself out”. I can’t wait while this country hits the repeat button on funding for models that don’t work and plans that don’t get executed my frustration rises.
My Non-Acceptance Disorder Professional Type is cycling up. My car rant therapy isn’t working.
Therefore,I will try a new treatment plan.
1) Write about it, topic of the day
2) Rant about it, car rant or otherwise.
3) Podcast on it. The #recoverycartel relaunch.
Today’s Topic:
History will look back on the manner with which the overdose crisis was handled, by treatment/#recovery/government/healthcare with a critical eye.
It will see 20 years of rising overdose deaths and our inability to contain this is an unprecedented public health failure.
Stubbornly adhering to unrealistic practices such as office based care, rinse and repeat #rehab .
Models founded on “wait for bottom” and “compliant client” paradigms.
One size fits all compliance programs and disregard for early stage substance use disorder.
Creating an incredibly high threshold for engagement of people who already don’t want to be engaged.
This country’s approach to SUD help is inhumane. It has always been inhumane.
These monster drugs reveal the gaps for what they are…deadly.
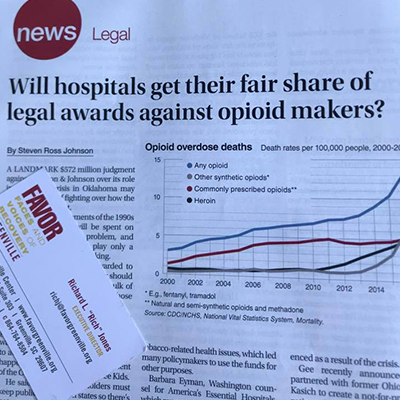
Check out this news-clip – See Picture Below:
FAVOR Greenville Will Fight
Big pharma money could be a similar mis-allocation. FAVOR Greenville is at the table w/legal team in SC.
We will fight for recovery services to funded at a substantial level and administered separately from other institutional systems. This will be another case where the money could be siphoned off.
Everyone will want a piece of the pie.
I hope people will share this post and people get aggressive about advocacy. Also, I hope people understand what I’m saying.
I do care what people think about me and I have no interest in personal disagreement. It’s all business right now.
At the end of the day this ranting process gets things out of my head.
Ideas for True Change:
To the federal government official person in charge:
1. FUND COMPETENT INDEPENDENT RECOVERY COMMUNITY ORGANIZATIONS WITH MILLIONS OF DOLLARS.
MILLIONS per organization. No nickle and dime crumbs.
Also, why continue to fund organizations that don’t actually deliver services?
Do we need more toolkits and committees or more boots on the ground?
2. STOP ALL CONFERENCES AND SUMMITS AND WASHINGTON D.C. CELEBRATIONS.
THERE IS NOTHING TO CELEBRATE. Re-allocate all money to direct services. Staff who do home visits, street outreach. Harm reduction.
3. FUND RCOs DIRECTLY. NOT THROUGH THE STATE INFRASTRUCTURE.
We need a Federal Department of Recovery separate from the single state authorities.
Keep funding the SSA at the same level (give them their overdue cost of living increases).
4. STOP ROLLING RECOVERY MONEY THRU TREATMENT AND PREVENTION PROVIDERS.
These are different things requiring distinct skills and philosophies.
5. INVEST MILLIONS
Invest millions INTO EACH QUALIFYING RECOVERY ORGANIZATION for 5 years. Not a $150,000 BCOR grant every year…..
Things today are not quite like the “Good Old Days”, but there are still echoes in the air!
One of the main reasons people struggle with accepting addiction as a brain disease or disorder is because we act like such complete a**holes when we the disease is active. We do nasty things.
Sometimes its dramatic and very obvious like breaking the law, neglecting children, stealing from loved ones, abusing people.
These are the hardest situations to reconcile.
Very hard to have sympathy for someone who hurts a vulnerable person, those in the middle of active addiction.
Sometimes the behavior is more subtle; but still way outside the bounds of acceptable human interaction.
CONSEQUENCES & PUNISHMENT
Our behavior in active addiction leads to the desire for consequences and punishment to be levied.
In the obvious ways like jail, losing jobs, losing our kids, etc…
However, it has also contributed to the punishing nature of many treatment and recovery approaches.
Simply put, people want to extract a pound of flesh from the addicted person.
IT IS YOUR TURN TO SUFFER
The addicted person made many people suffer so now it’s their turn to suffer.
This is why the industry can basically do whatever it wants in terms of housing and services.
The general attitude is “those bastards are lucky they have a roof over their head. Who cares if they are working for $1.43 an hour at the sausage plant and living 7 people to a bedroom”.
LIARS, CHEATERS & THIEVES
Even the addicted individual himself joins in the punishment.
I’ve been in group situations where people just one upped each other on how completely horrible they were in active addiction.
We call ourselves “liars, cheaters and thieves”. We think that people being hard and being confrontational is a good thing.
I get it. I really do.
THEY JUST DON’T WANT IT
I understand how things have evolved and how we have progressed to this point.
A point where we can ignore 90% of people in need because they “haven’t hit bottom”. They “don’t want it”, RIGHT???
These concepts work for the everyday person on the street.
Interestingly, this framework also worked for families for years but that has changed quite a bit.
FAMILY SUPPORT BASED ON ALANON
Remember, historically, the foundation for family support was based on Alanon which was (and still is) mostly wives dealing with chronic alcoholism.
Again, it was very natural for these wives to be somewhat hardened and “done” with their husband.
I get that as well. My wife certainly fit that criteria.
The program that was developed would reflect that dynamic. This may be a challenging fit, however, for parents.
I will make the following observations however:
1 – NOT GOING TO WORK
It’s just not going to work.
We can not punish or arrest or lecture or confront or debate our way out of the addiction crisis.
If it was a behavioral issue perhaps that would work. But we all agree this is a brain disease… right?
2 – OTHER WAYS OUT THERE
There are other effective ways to talk about to people about their issues.
An alternative approach requires more effort and it requires creativity.
It requires a willingness to talk differently, lecture less and be open to new ideas.
It means dealing with challenging people with a great deal of patience.
3 – CONFRONT & BREAK THROUGH DENIAL
Eighteen years ago when I started as a clinician I was literally taught to “confront and break through denial”.
However, I blew that shit off early on. I could see right away the damage that did.
The “hot seat” for example.
People who facilitated that group had to have a willingness to re-traumatizing people. I refused to do it and they kept me anyway because I was absolutely freaking exceptional at my job.
Then I got promoted and changed all that bullshit. Good times.
THE GOOD OLD DAYS
I do believe the culture of confrontation is slowly changing. However, if you pay attention, you can still see and still hear the ongoing influence of the good old days.
BONUS RECOVERY CARTEL INTEL REPORT
Please check out this article from Los Angeles Magazines blog, April 23, 2018.
It is possible, actually it’s likely, that the delivery of addiction treatment and recovery services will change at a fundamental level. The acute care model, as it currently stands, will essentially go away at the private level. It may endure at the government/publicly funded level.
One macro-level reason—the attention on the opioid crisis has lead to evaluation of the industry for the first time in history. White middle class kids started to die and people in the general public started questioning practices.
We are at the very beginning of that “questioning” process. Watch as the anger grows.
There are so many questionable practices to question.
I’m talking 5 to 10 years from now. Not tomorrow.
Driven by reimbursement policy, emerging best practices, emphasis on value based care, population health, and the horrible results of destination rehab. Most treatment will be local. The end of the destination rehab is near..
Out of network insurance reimbursement continues to change and is becoming more and more unpredictable.
The days of throwing millions of dollars in billing against the wall and seeing what sticks are numbered.
Less and less is going to stick. (ACA was an illusion) Revenue cycle management more difficult.
This, along with “local” treatment emphasis, will lead to hundreds of centers shutting down. The big boys will survive. And some niche boutiques. But the Walmart rehab days are limited.
There will be a push for addiction treatment services to be delivered and managed primarily through healthcare organizations. This will become best practice and standard of care. Further limiting referrals to the “drug and alcohol clinic”….. this discussion is already occurring nationally.
Professional Recovery Support services will become funded through diverse methods. CMS and commercial insurance will jump in because the cost effectiveness of the service too hard to ignore. Money talks.
As the model grows and gains momentum and validity. Imitation will run rampant. More “providers” leave the treatment fold and go back to running nursing homes.
Treatment Centers will then attempt to provide Recovery Support Services rather than “clinical” services. Some will convert. Many will butcher it. This will further eliminate many of the instant experts and more programs will shut down.
Hospitals take over the primary deliver of addiction treatment and form partnerships with Recovery Support providers. This is consistent with the management of other chronic diseases (diabetes, asthma, heart health) and the culture of healthcare and infrastructure exists to support Recovery Support services.
The BUBBLE HAS BURST….
This happens in every industry. Fundamental disruption. Creative destruction.
Out of the dust and the rubble a new system will emerge and 10 to 15 years from now it will be the norm. Standard practice. The new system will become “just the way we do it”….
You heard it hear First….. it’s now documented.
#nostradamus | #theearthisround | #askblockbuster
✌✌✌SIDE NOTE…One Group that may avoid this process is government funded system. That system is a monopoly. Like public education it may be untouchable.
MY SECRET LIFE AS A MEDICATION ASSISTED TREATMENT (M.A.T) THERAPIST
I’m sure we can find people out there who know much, much more about medication assisted treatment than I do. There are people out there who understand the technical end of medication assisted treatment better than I do. What do I mean by the technical end? The neurobiological process involved with a partial agonist versus a full agonist. The process of initiating the medication, the appropriate dosages, what you can expect in regards to withdrawal symptoms.
There are certainly people who understand more about medication assisted treatment than I do in terms of running a clinic. This includes all the rules and regulations. How many clients can a doctor have on their roster? What are the rules regarding “counseling” and drug testing?
There are people who understand insurance reimbursement and the business model better than I do. There are people who know more about the status of prescribers and why we seem to have a shortage. There are also people who have personally been involved with medication assisted treatment and they know more about the lived experience of M.A.T. than I do.
However, there are some areas that I understand more than anyone on the face of the planet:
I know what it is like to be an “independent” therapist who specialized in working with people on medication assisted treatment within a recovery culture that was very hostile toward those on M.A.T. And I did in complete secret and silence.
From 2007 thru 2011 I worked with hundreds of M.A.T clients in western Pennsylvania as the opioid epidemic raged. Suboxone was being prescribed at a high rate and it was, relatively speaking, a new phenomenon. These patients were absolutely marginalized by the larger recovery community.
Truth is they were also marginalized by “traditional” treatment providers. I was an active member of Narcotics Anonymous at that time. NA dismissed suboxone as “being high”. They were not welcomed at NA meetings.
This short quote from NA will give you an idea of this problem.
“Our program of recovery begins with abstinence from all drugs, including alcohol.”
I remember watching this unfold and thinking “this isn’t right”.
But I did not have the courage to speak up.
I was too enmeshed in the group. I wanted the approval of people “ahead of me on the path” and had not yet matured in my recovery. I sat silently as people on Suboxone dealt with the stigma within the stigma. It may be slightly better now. This was 10 years ago. It was ugly, it was brutal.
At that time, the common practice was “dose and go”. Physicians from a wide variety of backgrounds were getting “certified” as buprenorphine providers via a 9-hour online training platform.
There were some stipulations regarding counseling but none of the patients were getting any real coaching or support. This is still the case in many practices today, however, I think it has improved. 10 years-ago it was truly the wild west and most patients were getting their script and nothing else.
Of course, this presented massive problems.
As I stated above, I was an active member of Narcotics Anonymous at that time. Attending daily meetings, sponsoring people, chairing home groups. This was western Pennsylvania where the heroin epidemic has been raging for 15 plus years.
There were countless people showing up at these meetings on Suboxone. And the honest truth about the situation is they were completely marginalized and shamed out of the rooms. I am ashamed of how I conducted myself at that time. I would not participate in the bullying that went on around Suboxone.
I didn’t directly make comments about Suboxone being a crutch. I didn’t make comments like “they aren’t really clean”. However, I would sit by silently.
You see, all organizations or groups operate via social following principles. People fall into line and adhere to the group norms. We do this because we want to be accepted and we want to fit in. Evolutionary psychologists tell us that it is a survival mechanism.
As we evolved and we survived a nasty world it was essential that we be part of a tribe. Being a loner or going against the crowd equaled death. Back then it was physical safety we sought via compliance and group think. Today we follow the tribe to ensure psychological safety. Either way it is hard-wired into our thinking.
That’s not an excuse for my behavior, but it is an explanation.
Keep the reality of social following in mind when you consider what it must be like to be a person seeking recovery via medication assisted treatment attending a recovery support group.
Imagine standing outside smoking a cigarette (which is basically medication assisted treatment in its own right) while your “peers” make comments about people on suboxone. The official literature evens states: we are a program of complete abstinence. People would run from the rooms; and we all know how dangerous it is to try and “do recovery” without supportive people in your life.
NOTE: IT IS RIGHT ABOUT NOW THAT SOMEONE BECOMES OFFENDED BECAUSE THEY HAVE SPONSORED PEOPLE ON SUBOXONE OR THEY HAVE BEEN PART OF A WELCOMING RECOVERY GROUP. I WANT TO ACKNOWLEDGE THAT THERE ARE PEOPLE WHO ARE OPEN TO M.A.T. HOWEVER, IN THE INTEREST OF RIGOROUS HONESTY-WE NEED TO ACKNOWLEDGE THAT IN MAJORITY OF CASES YOU ARE A SECOND-CLASS CITIZEN IF YOU ARE ON M.A.T. AND IT WAS 100 TIMES WORSE 10 YEARS AGO….
With this culture firmly entrenched around me I became more and more distraught about what I was seeing where M.A.T. was concerned.
And then people started dying; at alarming rates.
Now at this time I was a therapist working professionally in the clinical treatment realm. I remember thinking: “OK the recovery community is not going to embrace this. Certainly, the professional community would”.
However, as I explored M.A.T. with traditional treatment programs and outpatient therapists I quickly realized no one was working with these patients.
That’s when I went undercover…
When I decided to start a private practice specializing in M.A.T. It was small initially but steadily grew and I became an expert on working one to one with these clients. However, the entire time I kept this quiet. I never openly discussed this with my support group. I never advertised. I never promoted it among my professional colleagues.
HERE’S THE THING: THE STIGMA AROUND M.A.T. WAS SO STRONG THAT I WAS AFRAID TO EVEN ADMIT I WAS TRYING TO HELP “THEM”.
Now, 10 years later, I could care less now what fellow professionals think about me as I try and help people on M.A.T. I still hear professionals say things like “suboxone blocks the sunlight of the spirit”. Now, instead of being intimidated, I am appalled and stunned that these people are permitted to practice. I cannot believe this type of thinking passes the test in terms of treatment or healthcare.
I have also developed a healthier perspective on the integration of M.A.T. into the larger recovery community. First of all, I think things have improved somewhat in terms of groups embracing M.A.T. It is different in 2017 than it was in 2007. Although, the truth remains that the official company line in most groups is “abstinence” only.
In the recovery rooms you will be accepted on M.A.T. if it is “temporary” and your goal is to get off the medication in the near future. It’s more difficult if your treatment plan includes long term medication maintenance.
More importantly, It is clear that self-help groups bear no burden in adjusting the thinking around medication assisted treatment. These groups are voluntary, free, mutual support programs. They do not charge health insurance. They do not promote themselves as healthcare. Therefore, they have no ethical responsibility to adjust the message.
I may not agree with the way M.A.T. is handled but it is the group’s prerogative.
The burden falls on professional recovery services, treatment and healthcare in general. Treatment and recovery providers who refuse to adopt medication assisted treatment as a viable practice must rethink their philosophy. Treatment providers who refuse to include M.A.T. in their practice should not be eligible to treat opioid use disorders.
These organizations should be denied payment or licensure to work with opioid use disorders; they can stick to alcohol and other drugs but they are a major part of the problem where opioids are concerned.
We must find a way to professionally support these folks and acknowledge how difficult it is to follow traditional pathways. We must bridge the gap through recovery coaching. We need to be there when these people are told “you aren’t clean” so that we can talk them through the reality of the situation. We need to pick up the pieces for the dose and go doctors that are still up and running in many communities.
As for our organization, FAVOR Greenville, we welcome you with open arms if you are on M.A.T.
You are in recovery if you say you are in recovery.
Your involvement with our organization comes with zero strings and no hidden agenda. We will help you identify your personal recovery plan and your personal pathway to recovery; with or without medication.
We don’t care how you get better…we just want to see you get better. Let us help.
This line of work can be difficult and overwhelming at times.
I have actually heard some public officials who work in our addiction treatment industry say “don’t talk about the opioid crisis it will frighten people”. Classic denial at the system and institutional levels.
We need to talk about it. We need to be open about the depth of the problem. What will it take to stem the tide of addiction in our community, the region and the nation. When the final numbers are tallied, the Center for Disease Control (CDC) projects overdose deaths will exceed 60,000. At this point overdose is the number one killer of people under the age of 50.
Here in Greenville County overdose deaths topped the state at 79. Over 700 overdoses were reversed. It is likely that we are just beginning to see the epidemic manifest itself in the Upstate area. I hope I am wrong about this. In the meantime, we have alcohol continuing its rampage atop the list of destruction. Over 70 of our most serious health conditions can be traced directly to the misuse of alcohol. It is not a stretch to say that substance use disorders constitute the greatest public health challenge in American history.
We have support in place via treatment and recovery services. We have outstanding self-help groups available. We have an increase in options for treatment and we have made concerted efforts at breaking through the stigma. Yet the death rate continues to climb and our facilities are full. Many times, with the same clients over and over again. Recent research indicates that 70% of the people in treatment are repeat customers and only about 20% follow through on any programming following completion detox. We know we need to push the envelope of innovation where substance use disorders are concerned. We need to work hard at forging partnerships and we need to look outside the box to find these partnerships.
One such transformational collaboration has been unfolding over the past 2 years with University of South Carolina School of Medicineat Greenville Health System campus. The med school has welcomed FAVOR Greenville with open arms. We have presented on the topic of recovery on several occasions. Shared our stories of success and our struggles with addiction. It has been a great opportunity to expose future physicians to authentic recovery principles.
The relationship went to an entirely new level with initial FAVOR Greenville Recovery Coach Academy specialized week-long training for medical students. This 30 hours coaching curriculum is the only such training in the nation.
The comprehensive nature of the education and the collaboration makes the experience exceedingly unique and a model for healthcare across the country. We believe returning treatment services to healthcare will be a key part of winning the war on addiction. Fully integrated addiction treatment services will make a major difference in turning this thing around. We are very grateful for USC-Med School @ GHS and especially Lauren Demosthenes for making this possible.
We also believe that this symbolizes a much need paradigm shift. The med students in this class were exceptionally compassionate and open to helping people with substance use disorders.
It made me think: “perhaps these are the partnerships and healthcare is the pathway to transformation”.
If the medical field truly embraces addiction as a healthcare issue, the stigma will take a direct hit. As it currently stands, we know that most doctors do not address substance use disorders directly for a wide variety of reasons. The group we trained seemed to be wide open to having the necessary conversations. Most importantly, there was zero stigma or judgement in the classroom and this is a very hopeful development.
Over the next year, these coaches will serve as volunteers and support FAVOR Greenville as we work toward connecting with participants across multiple healthcare venues. The potential benefits are limitless.
“It makes us wonder…what exactly will we accomplish if healthcare becomes the first line of defense in the war against addiction.”
1.INCREASED IDENTIFICATION and EARLY INTERVENTION:
The most obvious benefit is INCREASED IDENTIFICATION and EARLY INTERVENTION. Healthcare workers are on the front lines of this addiction crisis. They are faced with the obvious and subtle effects of addiction all day, every day. Therefore, empowering healthcare staff with the tools to identify and engage patients in the recovery process is essential. There are efforts underway to implement Screening Brief Intervention and Referral to Treatment (SBIRT) within many healthcare facilities. SBIRT is evidenced based and, if utilized, can make a difference. Getting buy in and full implementation is another story. This has historically been a very difficult process. We believe increased knowledge of recovery options and partnerships with recovery organizations can help fill in the gaps that exist in the SBIRT system.
2. ADDICTION IS A DISEASE:
If we actually handled addiction in the healthcare system, rather than off at a designated (sometimes isolated) drug and alcohol clinic, the stigma will be reduced. It is also more likely that addiction will be viewed as a disease by the general public. Hospitals and healthcare systems; this is where disease is addressed. Of course, there will always be a need for some specialized rehabilitation centers; just as there is specialization in other areas of healthcare. However, we could eliminate at least 50% of the “treatment centers” and roll those services into the healthcare system.
3. TRUE HOLISTIC CARE:
If done well, co-occurring mental health and co-occurring physical health issues could be addressed within the same system as addiction. This seamless coordination could improve overall outcomes. There would be a synergistic relationship where physical health contributes to improved behavioral health and vice versa.
4. VALUE BASED HEALTHCARE:
Although it is not a guaranteed thing in today’s uncertain political climate, value based healthcare seems an unavoidable reality. This would be a transformational development if applied to the addiction treatment world. Creating an environment where programs were held accountable for patients returning to treatment over and over (rather than rewarding programs for rinse and repeat) would change things over night. Challenging and disrupting the current business model may be the single most important challenge we face. If addiction services were housed within healthcare it is more likely that value based healthcare would be applied to treatment services. This is reason enough to move toward healthcare integration.
5. EVIDENCED BASED TREATMENT:
Much of professional addiction service is guided by conventional wisdom and traditional values. Some of this is very helpful. Some of this is very problematic. Most centers operate from a 12-step only model that lacks evidence. The move toward alternative programming has been hampered by pre-existing practices that are very entrenched and difficult to move. There is too much tradition to impact significant change. If we moved addiction service to healthcare it would increase the likelihood of evidence based treatment because healthcare is not beholden to any traditional framework. We could start over and we could promote multiple pathways to recovery.
6. WE COULD ELIMINATE THE “HUSTLERS”:
As we know we live in the age of “instant expert”. If you are clean and sober for a couple of weeks and you can get a treatment center to pay for your Facebook ads you can become a marketing machine. The industry is full of hustlers, and the hustle is working.
The people who are considered experts in this industry are, in many cases, harmful actors with little knowledge and lots of con. It stands to reason that, If healthcare was responsible for inpatient treatment services, and we could eliminate much of the private treatment market. And these hustlers would have to go back to selling junk bonds.
As stated previously, it is likely we will always need some form of rehabilitation. However, our current approach has shown itself to be inadequate as best. The rising death toll, the dismal retention in services, the low treatment engagement rate, and the 70% rinse and repeat reality make this clear.
Why not transform the system by bringing professional clinical addiction services under the umbrella of healthcare?
Or we can keep doing what we are currently doing, over and over, and expect different results.
Will we try something fundamentally different when 100,000 people a year die?
6 PRINCIPLES THAT WILL TRANSFORM THE RECOVERY WORLD
“Cartel–an arrangement between parties to promote a mutual interest or goal… “
I believe it will take a RADICAL reshuffling of the current treatment approach & public policy to make a dent in this crisis. I say this because all our efforts, so far, have fallen short as indicated by the astronomical increase in over-dose deaths. If it’s a disease the primary indicator of successful care would be keeping people alive. Right?
All that we have done to this point has been predicated on our pre-existing approach/philosophy. All our money and resources have been funneled through our pre-existing system of care.
It’s going to take a massive shake to transform and usher in change. Our institutions will double down on current practices. Because that is what institutions do. They exist to sustain themselves. It’s a sociological fact.
The change could come via the free market. If treatment providers saw the wisdom of a new business model. However, that would only happen if current business dried up. “If it’s not broke don’t fix it”…. seems to be the prevailing philosophy. And I don’t see it drying up soon. Too deep a problem. Too much demand. Plus 70% repeat business makes the model self-sustaining.
The solution will come via “outsiders” AND NON-CONFORMISTS. Independent thinkers, people from other industries, progressive healthcare providers, and risk takers. Partnerships that, on paper, make little sense but in practice lead to transformational ideas.
THESE PARTNERSHIPS WILL PRODUCE RADICAL IDEAS. People will actively push back on the ideas. When that happens, it indicates that the proposed idea is probably the right type of idea…bureaucratic objection especially, is a litmus test for a great idea. Almost as promising as when a treatment provider tells you “that’s not the way we do it”…. then you are on the right track.
It’s going to take a cartel…A RECOVERY cartel. Like any good cartel we need to have our organizing principles and our mutual goals… From my perspective the CARTEL holds the following principles near and dear.
Within the CARTEL we embrace the concept of “keep coming back”. For us, this is not just a cliché or a theoretical ideal. For us, it is the measure of our success and the single most important aspect of the recovery process. We know that people who stay engaged in a recovery process, regardless of the specific pathway, tend to get better. Even if you struggle along the way your life starts to improve. Even if you “mess up” and use, things begin to get better. Furthermore, we believe that the vast majority of people that continue to work a recovery program do eventually sustain long term recovery.
On a very practical level this means we will never preach to you or judge you. It means that we are all on equal footing in terms of our recovery. It means there is no hierarchy of recovery or right or wrong way to do recovery. We don’t count days. We don’t prescribe specific pathways. We just want to see your life improve. We just want to see families get put back together. We will meet you where you are in this process. If you are still using our goal is to help you figure out next steps and how this behavior fits in with YOUR personal values. Not ours. We have no agenda other than your welfare.
We believe substance misuse is a healthcare issue. We offer you a place to discuss it as a healthcare issue. It is not a moral failing. If you are struggling with substances you probably have considered stopping. You may have tried before. We believe we can provide you with new information, supportive coaching and unconditional positive regard.
Our core recovery principles include the following:
1. You are in recovery if you say you are in recovery.
Admittedly this philosophy is NOT exclusive to the CARTEL. Many other recovery community organization have adopted this perspective. I have been in situations where the definition of recovery has been a hot topic of debate. I have been in situations where people have contested the merits of the term “in recovery” versus the term “recovered”. I have little tolerance for such things.
Entering into recovery is a difficult process. If we make people stand at the threshold and question if they “qualify” it is only going to drive people away. Therefore, for our purposes remember…you decide if you are in recovery. No need to fill out an application or get your passport renewed. You’re in.
We hope to assist you in the journey and we know that recovery is process not an event. If we offer advice and support it is in the spirit of guidance and it comes with unconditional positive regard. We stand in radical non-judgment of your journey. However, we will tell you if your ship is sinking. We will just do it in a very loving and caring manner. No shame. No punishment. No judgement.
We want to welcome you to recovery, regardless of how you define recovery!
Recovery is NOT a contest…
2. There are multiple pathways to recovery.
Again, this may not be earth shattering. As a matter of fact I hope people read this and say “of course there are multiple pathways. My fear is, there are many who believe that there are only specific ways to recover and any effort outside of that framework is futile, inferior and doomed for failure. I used to think that way. What a horrible outlook on recovery that was.
“Rather we shall reflect that the roads to recovery are many.” – Bill Wilson Co-Founder, Alcoholics Anonymous
People find recovery through countless avenues. Research indicates that the majority of people with a diagnosable substance use disorder will recovery via a process of “natural” recovery. In other words, they will find ways to eliminate their substance abuse and live a productive life without formal intervention and formal “recovery programs”.
I do not dispute this research. However, I have concerns with waiting for people to “figure it out”. In this age of overdose, we need to be very aggressive, assertive and effective in promoting recovery. That said, the key part of the message needs to be multiple pathways exist and you can invent your own pathway. We just believe that you can get that done more effectively if you have a coach or a mentor to help you figure that out.
Recoveryism is a term that has been used to describe the phenomenon that exists where people hold the position that their personal path of recovery is the “best path of recovery”. Actually, many believe that their personal pathway of recovery is the ONLY pathway of recovery.
This is a most dangerous form of tribalism. Can you imagine how many people have been alienated or chased away via such attitudes? There is no legitimate place for this in the recovery world and certainly should be ZERO tolerance for this in the professional community.
3. You should not be required to “quit” prior to becoming involved in a professional program. The person who is “not sure” what they want to do with substance use, has a right to, support, coaching, and direction.
Change happens across a predictable and universal process. The stages of change have been well researched and validated over and over. They apply to anyone making a behavioral change including someone dealing with a substance use disorder.
Many people struggle with commitment to change and a constant process of “thinking about” change (ie. Contemplation stage). This is completely natural.
Most programs require “willingness” and will only work with the person in the action stage of change. We believe, instead, that working with a person in contemplation is just as important as working with the person in preparation or action.
We also believe that many people in contemplation will move to preparation and action if they have people to talk to about the issue. Processing information about the change moves the person through the change process. Isolation does not.
Therefore, we would love to see you even if you are not sure you want to quit. Even if you are not sure you are an addict. Even if you want to come to just get the heat off for a little while. We will help you get the most out of your experience.
4. We believe family recovery support is also a primary part of the process.
Family recovery stands on its own merit and should be available regardless of the status of the addicted loved one. Some type of recovery plan is essential for all family members. We know that family members can benefit and experience improved mental health, reduced stress and ostensibly better overall physical health. Therefore, the primary purpose of family recovery is improved health and welfare of the in and of itself.
However, we have observed an interesting phenomenon. When the family takes “care of itself” the addict frequently follows suit. This has been validated by a wide variety of resources. ARISE intervention model teaches this very philosophy. It was in my ARISE certification training that I first heard the statistic “1 family member is as powerful as 8 professionals”. Additional studies have been done on the impact of the family. Behavioral couples therapy for example has been shown to deliver around 66% success in getting the addicted individual into services.
Very important: Tough Love is an oxymoron. YOU NEED TO FOCUS ON APPROPRIATE EXPRESSION OF LOVE. NOT TOUGH LOVE. Sometimes, setting limits and boundaries is the appropriate expression of love.
We do not believe in complete disengagement. Many things you hear about family role in recovery are dangerous.
WE HOPE TO DISPEL THESE MYTHS.
5. We believe that recovery is a process not an event
We know that, statistically speaking, it takes on average 4 or 5 genuine attempts at recovery before “it sticks”. This isn’t to say relapse is a necessity. It is not. However, relapse is nothing to be ashamed of and should be met with loving compassion. There is a need to make “returning to recovery” as easy as possible.
We also believe that professional services that specialize in re-engagement are essential to the continuum. There is a glaring hole in our professional service structure and we need to provide long term support. We need to re-vamp our system to support long term, chronic disease management rather than episodic acute care.
6. And finally…we believe RECOVERY will bitch slap addiction if we allow it to.
If we come out of the shadows and conduct ourselves as responsible members of society the community will embrace us. If family members become open about their struggles the community will embrace them. There is power in numbers.
However, our efforts in this area have been set back by “advocates” who reinforce the stigma when they speak for recovery. Much work has been done on messaging and identifying the most effective way to carry the message. Market studies have been done. Focus groups have been conducted. There is productive way to share the message of recovery and there is a counter-productive way to carry the recovery message.
A public lead meeting or online speaker meeting is not the way to promote recovery. This type of spectacle works for those already in recovery. However, we are not trying to preach to the choir. We are trying to reach the masses. If the goal is true advocacy then please adopt some type of intentional recovery messaging.
If the goal is to fill your treatment center than keep doing what you are doing.
However, in the interest of “rigorous honesty” please give up the word advocate.