Constant connection into social media leads to constant comparison.
The picture above is from a Psychology Today article title “The Comparison Trap”. It outlines the diabolical dark side of social media.
For many people this constant comparison leads to an ever-present nagging feeling they may be falling short in their own lives. Human beings are hardwired to assess how they measure up.
Human beings are subconsciously drawn toward assessing their status within the group.
This Self Assessment was essential for survival as we evolved.
If you weren’t accepted and of low status back in the day you were in danger. Being a central and valued part of the tribe meant physical safety.
Today we seek acceptance and status to preserve psychological safety more than physical safety.
Social media is most damaging to those who are most actively engaged.
Young people are most vulnerable to issues associated with status seeking.
Think about being in middle school 24 hours a day 7 days a week. Never able escape the cliques and the constant message “you aren’t cool enough or pretty enough etc…”.
Social media is not the only factor contributing to our current societal crisis.
However, it is clear that social media has had a significant anti-social impact. Being able to look at pictures of those with perfect personal lives and epic professional accomplishments can chip away at self esteem.
Pictures that are perfectly produced with just the right angle and just the right filter.
One problem we face and that we can not ignore. We can never really tell how well a person is doing “in their Recovery”.
We can usually tell if someone is not on solid ground.
Obvious signs like: not attending meetings, not going to therapy, running with old using friends, dope man on speed dial.
LOOKS & SOUNDS GOOD
But what about the person who appears to be on point? The person “working a great program”.
Attending to all aspects of the recovery plan. Everything looks and sounds good.
I believe you can be doing all the right things and still be struck with a strong craving.
Especially where opioids are concerned. Especially during that first year.
❌STOP – WAIT
Before you say it allow me:
1) I fully understand that sometimes we just have to get through the craving and “not pick up no matter what”.
2) I fully understand that the person can call and “tell on himself” and work through the craving.
3) I also understand that some people feel that the obsession to use will be lifted and they won’t face this type of circumstance.
But I also understand that in many cases, perhaps the majority of cases, the person won’t take action.
I also believe many people aren’t “free” from these moments of weakness.
Especially in the first year.
THAT FIRST SLIP
Some people will give in and make a mistake.
Conventional wisdom tell us to wait and see “if they make it back”.
Then we can use the mistake as a learning tool.
And encourage the person to try again, to “keep coming back”.
An approach consistent with the “wait until they hit bottom” foundations of our system.
THE SLIP IS FREQUENTLY FATAL
In another day and time we may have been able to get away with this approach.
The mistake was not likely to kill the person on that first “slip”.
But in the day and age of carfentanyl and fentanyl the slip is frequently fatal.
And a person who has been “clean” for a period of time is in the greatest danger because tolerance is low.
Who among us has had a perfect recovery? A spotless trajectory of no lapse or relapse?
Who got this on the first try? Very, very few of us.
THE ARGUMENT FOR M.A.T.
When I made my mistakes that first year I was not in imminent danger. And I had a chance to make it back.
There was no fentanyl to be had.
Death was always a remote possibility. But not a probability like today.
This where the argument for MAT is most compelling.
ZERO WIGGLE ROOM
Even if a person is following a traditional recovery pathway, perhaps the adjunct of MAT makes sense that first year. When cravings are frequent and relapse deadly.
Even the person working a “great program” could benefit from the added safety net of MAT.
There is just zero wiggle room where heroin and other opioids are concerned.
More likely legislators with influence over FDA. Probably FDA directly.
IT’S THE ILLUMINATI ???
I’m not saying there is some Alex Jones Illuminati type stuff going on; but if you think our government is pursuing justice and truth you are silly and naive.
And this crony capitalism is not confined to any one party. Sometimes it has nothing to do with political party. It’s the regulatory body itself independent of legislators.
TRUTHS AND NORMS
This false evidence presented as real shows up in all societal institutions.
Religions, legal system/prison system, school system, military and all the other major institutions of society have their own galvanizing indisputable truths. This is what makes the institution function.
Furthermore, from a functionalist perspective, these institutions reinforce the facts put forth by other institutions because it holds everything together. Society “functions” better when all agree on “truth and norms”.
EXAMPLE #1 – RELIGION
Example: Religion has always been used to reinforce civil norms and encourage obedient behavior. In all religions and all countries it’s part of the equation. Sometimes very overt. Sometimes more covert and deceptive.
EXAMPLE #2 – DRUG LAWS AND THE INDUSTRIAL PRISON COMPLEX
Another Example: drug laws are used to perpetuate the industrial prison complex.
—The United States locks up a lot of people.
Our prison population rate of roughly 700 per 100,000 is the second-highest of 222 countries tracked by the Institute for Criminal Policy Research.
Private correctional facilities were a $4.8 billion industry last year, with profits of $629 million, according to market research firm IBISWorld. Yet we “must protect our youth from the evil drug dealers”. ALL SUPPLY SIDE INTERVENTIONS ARE DOOMED TO FAIL.
EXAMPLE #3 – THE ADDICTION TREATMENT SYSTEM & THE RECOVERY MOVEMENT
—Another example: the indisputable “truths” which hold together our addiction treatment system ($46 billion industry) and our evolving centralized “recovery movement”.
TAKE NOTE: APF and their underlings are trying to “control” the movement; including the allocation of funding.
If you think ALL the “experts and gatekeepers” at the front of our “Recovery Movement” are putting forth pure objective unbiased info you are truly naive.
NOTE: I have great respect and admiration for many people and organizations in the Recovery space.
Even if I don’t agree with the others I know they aren’t bad people. They simply have an agenda and think they know best.
WE ALL DESERVE TO KNOW THE RULE OF THE GAME
APF tried to sneak in $10 million in Self Funding through legislation that we all fought for. Money that the entire “Recovery Movement” fought for.
By and large the “Recovery Movement” has been silent. Aside from some brave voices who are willing to walk their own path. Everyone else appears to be toeing the company line.
As a matter of fact I am starting to think I must be foolish for being upset about this.
It appears everyone else in the “movement” is cool with APF’s private deal. One thing for sure. This new recovery “thing” is certainly not a movement. It’s an evolving system and a burgeoning industry.
Or more accurately, an off shoot of the treatment system. History repeating itself.
That’s fine. But we all deserve to know the rules of the game.
PUNCHED IN THE GUT
APF doesn’t represent FAVOR GREENVILLE worldview.
When FAVOR GREENVILLE advocates for legislation and recovery money WE DO NOT support any of it being allocated to “literature and training”.
We had no idea that was part of the plan. This isn’t the first time FAVOR GREENVILLE has been punched in the gut.
In February 2018 I participated in an event in Washington DC that was broadcast-with the surgeon general; and some members of congress.
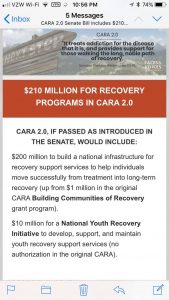
At that event we (the recovery movement) officially requested $220 million.
Shortly after that event Faces and Voices/ARCO sent out an email celebrating the fact that Sheldon Whitehouse (senator) seemed on board and the $220 million request stood.
STAND UP FOR ITSELF
The recovery movement was finally going to stand up for itself and not just advocate for more money for treatment and the legacy provider system.
As the legislative process unfolded APF sent a letter to Congress proposing allocation of money in CARA 2.0 legislation.
It detailed where APF recommended the money go.
The amount allocated to recovery support (places like FAVOR; recovery housing etc…) was $7 million of a $4 billion proposal. $7 million instead of $220 million.
Furthermore, the APF letter that was sent to congress included a section that stated this request is supported by over 100 recovery organizations nationwide including the following: it then listed all the ARCO members. Including FAVOR Greenville
OVER-SIGHT OR MISCOMMUNICATION ???
I would have never signed off on those changes.
We were never ask about our support for that allocation. Not by APF; Not by Faces and Voices national.
I never said I agree with the APF document.
I never got the opportunity to review the document ahead of time. And when I did review it (after it was sent to Congress). I didn’t agree with much of it.
Perhaps it was oversight. Perhaps it was miscommunication.
CANNOT CONCEIVE
However, I can not conceive any circumstance where I would have the hubris to speak for another organization without written consent.
NO ONE SPEAKS FOR FAVOR GREENVILLE AND OUR AFFILIATES EXCEPT ME AND OUR BOARD CHAIR.
On one hand we are very frustrated at FAVOR GREENVILLE.
On the other hand it is good to have clarity and realistic expectations surrounding national advocacy.
NO INTENTION TO FUND
There is no intention to fund independent recovery supports.
It would not be politically expedient for APF and their associates to pursue such radical ideas. They will bank on toolkits and blueprints and resource lists. Much safer and acceptable to the status quo.
WE INTEND TO GAIN PROMINENCE
At FAVOR GREENVILLE we intend to gain prominence nationally based on merit and performance and winning in the free market. We know we won’t be invited to any advocacy awards dinners and we may be kicked out of the “club”.
However, we have realized that the the world outside the recovery bubble loves us and is willing to be part of the solution. Corporations, healthcare systems, benefits administrators, and the technology industry are willing partners.
WE KNOW WE CAN DELIVER
They judge us based on performance and value add. That makes us hopeful because we know we can deliver.
I would have stayed in the treatment system If I wanted to struggle with arbitrary gatekeepers and “experts”. It’s hard to abdicate authority to people who have never executed in the actual delivery of professional recovery services.
We have no intention of following people/organizations/protocols which operate mainly on theory.
Or worse organizations that just repackage the 60 year old treatment system.
I have little time nor tolerance for theory over practice.
I will follow the lead of people who add value and get things done effectively on the ground in direct service.
ACCESS TO UNLIMITED INFO
In modern society we have access to unlimited info. The isn’t 13th century feudal system where we have no info and we just need to accept that the king’s rule is “divinely ordained”.
Read. Educate yourself. Check out other sides. Access your own critical thinking. If you are in the “Recovery Movement” take time to investigate. Don’t blindly follow the herd.
For that matter. Challenge me as well. I’m not an “authority”. I just have an opinion.
Tell me how I’m wrong. Tell me where you differ.
Let’s talk!
RICHARD JONES MA, MBA, LCAS, SAP EXECUTIVE DIRECTOR 864-764-8504 (cell)
THIS IS AN OBSERVATION BY RICH JONES | RECOVERY CARTEL
It sounds sarcastic and provocative but it’s truly an observation. And the points I make are unassailable.
I challenge someone to tell me what I’m missing.
With the facts below in mind, understand that the long standing manifestation of treatment/“rehab” is unsustainable.
The approach used to get customers is so insanely one dimensional and insulting to the average human being that it is unsustainable.
ONLY 10%
No wonder only 10% ever show up for treatment.
The reason it has lasted this long is the stigma.
No one in the outside business world wanted in on this industry because it’s a stigmatized patient group. No one creative considers involvement because those “scum-bag” addicts are an afterthought.
A NEW BUSINESS MODEL
Historically, if an outsider does decide to get in they just followed the rehab formula because it was a proven business model.
No one bothered thinking about creative destruction and inventing a new business model.
As stigma is reduced and awareness raised more and more outsiders will become involved. And things will change.
A new business model will emerge.
Marketing in the addiction Treatment/Recovery industry is really only focused on filling rehab beds and appears to fall into one of 8 categories/strategies; or a combination of these strategies:
8 CATEGORIES / STRATEGIES
Hire someone/maintain team to do face to face business development to outpatient, doctors, etc…. focus on legacy relationships, brand and reputation to fill beds. Use outpatient clinics to funnel clients as appropriate. This is mostly used by the large legacy programs and integrated massive systems.
Digital media (Facebook, Instagram etc…) with the apparent strategy being create a persona or use pseudo-celebrity/actually celebrity to basically tell his/her 12 step story over and over….while encouraging people to call now for help.
Digital media where these same personas, pseudo celebrities/real celebrities diss other pseudo celebrities etc…. while encouraging people to call now for help.
Digital media where these pseudo celebrities etc….tell parents they are enablers and killing their kids….while encouraging people to call now for help.
Google ad-words at hundreds of thousands of dollars per year.
Annual conferences (NAATP, C-4 etc….) where people talk about the latest innovation in treatment and ethical marketing practices. While encouraging one another to “keep us in mind if you think you have a fit for our program”….
Some guy in doctor scrubs on television in the lowest production value commercial in the history of TV encouraging people to call now if you or a loved one need help.
Body brokers.
With the exception of number 1 and number 6. The content of the marketing message, despite the platform or avenue of delivery, is essentially
“You’re hopelessly addicted. You’re in denial about that. Call now and get help. Or you’re gonna die”….. or
“You’re loved one is hopelessly addicted. Get your shit together and stop enabling. Call now or they are gonna die”…..
Number 1 works because the narrative of “we are the expert healthcare providers/treatment providers and state of the art etc….” and “we are really you’re one best option” has never really been challenged.
Legacy and brand is hard to overcome.
Number 6 is just an excuse to visit a posh resort and play golf. 😎😎😎😎
This is an industry that is going to get completely turned upside down as soon as the knowledge of the issue (and the associated opportunities) escapes the Recovery Bubble. Begging for disruption….moral imperative to do so.
Who is thinking about the behavioral health crisis in a visionary way in hopes to solve the epidemic.
Overdoses and suicides #1 and #2 in injury related deaths respectively. Anxiety, depression record setting levels.
Consider this…
Flat-Earth?
In order for people to discover the new world they had to allow for the possibility that the world was not flat.
Einstein proposed particle theory at a time when all scientists were certain light was a wave.
The American Revolution (1775-1783) took many ideas from the early civilizations of Greece and Rome and combined them with the Christian Bible to revolt against an authority that was unbending by embracing a completely new concept: a modern representative republic.
Gutenberg invented the printing press around 1440 changing the way that information is disseminated and changing the world. Before this monumental creation books were copied by hand and humans were limited in their ability to transform their lives/move beyond their immediate sphere.
The industrial revolution, the assembly line, the invention of the automobile ushered in a new era of urbanization and economic growth.
Steve Jobs decided it was possible to put the power of a mainframe computer in our pocket.
The internet has made instant access an everyday mundane experience.
Elon Musk is trying to solve the LA traffic problem by tunneling under the city. It looks like it will work.
We could go on and on… in each case the world changing development required visionary thinking.
Over the past few decades, practitioners and researchers increasingly have recognized the link between substance abuse and mental disorders. Some studies suggest co-occurring disorders are present in up to 60% of addiction treatment admits.
Defined as the presence of at least one substance use disorder and at least one axis 1 mental health diagnosis or axis 2 personality disorder. Some states have aggressively pushed COD services.
Clinical credentials reflect this commitment to COD services—for example:
I am a Certified Co-Occurring Disorders Professional from my days in Pennsylvania.
Treatment Improvement Protocol
There is also a SAMHSA guide called TIP 42 (Treatment Improvement Protocol) that serves as guidelines for COD services.
When it came out in 2010 (?) there were also TIP 42 trainer the trainer courses.
I am a Certified TIP 42 trainer (talk about an obscure credential).
Facilities in PA could also become accredited as COD INTEGRATED (the highest standard) or COD COMPETENT clinical facilities.
The hope was that COD services would become the norm. This “movement” has lost much of its momentum.
I am of the opinion that the mismanagement of COD issues is the second most dangerous issue facing individuals and families seeking help.
Behind only straight up body brokering.
The 4 Quadrants
COD comes in many different manifestations
Q1—Quadrant 1: LOW Mental Health/Low Substance Use Disorder Q2—Quadrant 2: LOW Mental Health/High Substance Use Disorder Q3—Quadrant 3: High Mental Health/Low Substance Use Disorder Q4—Quadrant 2: High Mental Health/High Substance Use Disorder
1-800 CALL-CENTER
The problem is when someone calls your average addiction treatment “helpline” or “treatment line” hey will almost automatically be pushed toward rehab. (They almost diagnose the problem with little or no MH training or education.)
You hear it all the time.
A mantra of get them into detox, rehab, long term residential care.
There may be a sense that having a psychiatrist on staff will take care of the possibility of a COD.
That’s woefully inadequate.
If it is a Q1 or Q2 issue it would be no harm no foul. Much of that can be handled.
Very Specialized Care
If it’s a Q4 issue you need very specialized care. The most troubling is a Q3 (high Mh/low SUD).
Many times a family member will call an addiction treatment program with a Q3 situation because it looks like SUD may be the problem.
When in fact it is a symptom of the primary mental health issue.
A great example of this is breakthrough mania associated with bipolar type 1.
The mania frequently involves a wide array of risky, impulsive, dangerous behaviors that could include out of control drug or alcohol use.
More Harm Than Good
And it is possible that taking a person with true bipolar type 1 and plugging them into your standard addiction treatment setting results in more harm than good.
Again….having a psychiatrist on staff does not mean it’s competent the effectively work with co-occurring Disorders.
Require Competency
To be COD competent require competency in skills training, working with families and case-management directly related to the mental health issue.
Telling a Quadrant 3 client that their aftercare plan is attending an intensive out-patient, and go to 90 meetings in 90 days, is….. well problematic at best.
Be Extraordinarily Careful
YOU OR YOUR LOVED ONE IS HIGH MH (Q3 or Q4) you are better off in a MH primary facility if there is no COD competent program.
I fully understand that access to integrated COD and competent COD facilities is lacking.
And many people can’t afford top notch COD care. In those cases you may need to piece together a solution.
Please understand if you call one of the “get help now” phone lines you will be steered to addiction treatment. If Q3 or Q4 is your loved one’s reality you must be extraordinarily careful.
✌️✌️✌️It will be necessary, in my humble opinion, to engage technology fully in addressing substance use disorder and mental health.
Our front-line, first response to these issue can not continue to be waiting for willing people to go to rehab or waiting for willing people to wake up and see a psychiatrist/therapist.
These traditional providers could could continue to play a role in a brave new behavioral health world. There will no doubt continue to be some willing folks “show up” and adhere to “treatment plans” (10% in SUD; tops 30% in MH)
However, full engagement of technology will be necessary to stem the tide of overdose, alcohol related deaths, suicides etc… (Deaths of despair).
Artificial Intelligence
Society uses machine learning and artificial intelligence in every aspect of life.
Data collection and profiling leads to internet platforms that anticipate your needs and send you a pro-active advertisement. It’s as if “they” are reading our minds.
I’m not saying this is a good thing. I think the ethics of “big data” is yet to be hammered out. But I am saying it’s noteworthy.
Could technology be used to a) engage more people in need; tap into this data; profile and send pro-active messages of support. Maybe even intervene.
There are companies already exploring this possibility. b) provide base level coaching?
I know you are going to flip out and say “counseling can only be done face to face; counseling requires a human interaction”.
Identify Common Themes
Here’s my response. Yes; there are issues that must be addressed through a traditional setting. More serious, deeper issues. Trauma for example. But after 18 years of mental health and addiction work I could identify some common “lower level” themes that could be addressed.
Furthermore, people are NOT showing up to address these base level emotional issues because it hasn’t “gotten bad enough yet”. Easy access and engaging technology would put a dent into these unaddressed issues. c) as stated above identify at risk people and pro-actively intervene.
Big Brother Type Stuff
There are many objections that can be raised. There are many reasons not to do this. This sounds creepy. It sounds like big brother type stuff. But the big brother type stuff is already happening.
The difference is they are using the data to sell you a $3 t-shirt for $75.00. They are using the technology to successfully drive consumerism. Could technology be used for noble reasons.
To solve the number one public health issues facing America; Untreated mental health and substance misuse.
Time and Money
Another barrier is cost. Full engagement of technology requires massive investment in time and money. It’s not something you throw together on the side and it goes way beyond a monitoring system/app.
✌️✌️✌️The Demi Lovato overdose has really brought out a bunch of “experts” to tell us the ins and outs of addiction. Who are the gatekeepers that arrange this stuff? How do they pick the “expert”… have any of them actually worked with a person with SUD or with families?
It may not matter because the media is looking for a cliche and a sound bite. And those are easy to come up with. The “expert” can deliver that.
But is all this attention and noise thrown Demi Lovato’s way good for her? Or good for society? I guess it’s good for the “experts”.
The Circus Has Come To Town
It a freaking circus. My home page is Yahoo News and here are a couple of stories that popped up over the last few days (I’m paraphrasing)
1) Demi Lovato overdosed because she bought into the “moderation” lie. With some idiot proclaiming with authority the abstinence only dogma. Like they know everything about Demi Lovato and why she overdosed.
2) Demi Lovato overdosed because she “gave up”… well damn…. they seem to have figured that out from some song she recorded about 6 months ago….geniuses.
3) Demi Lovato overdosed because of a “negative body image”…..HOLY MOLY! There must be Jedi therapists out there who can evaluate people from afar and make precision diagnosis.
Y’all depress me. You aren’t experts. You don’t know anything about Demi Lovato. Y’all should turn down the interview. It’s not a sideshow. It’s someone’s life. And it’s damaging to all people seeking recovery.
When a celebrity has a recurrence of cancer is it publicly announced and scrutinized? Do they evaluate “where it went wrong” what the celebrity patient did wrong leading to the recurrence?
This is par for the course for the media. But the “recovery experts” should not contribute. It’s not good. It’s not “awareness”. This is not “advocacy”. It’s a circus.
Do we really need to continue with the Make the Addict Suffer Model?
Or is there a better way?
I have been trying to make sense of non-sense. I have a rambling theory….about 18% to 20% of people with SUD are also narcissists and sociopaths. A much higher percentage than the general population.
Perhaps this lead to the common punishing tactics used in treating this issue.
Narcissists and sociopaths will only respond to clear consequences and “tough” boundaries. You don’t LOVE a narcissist into Recovery. You paint him or her into a corner and they have no choice.
So the hard-ass stuff works on this group. BUT, stating the obvious, the overwhelming majority ARE NOT narcissists and sociopaths.
This group will actually be harmed by the hard-ass approach.
They Love You!
The media also LOVES THE NARCISSISTIC story line. Reality TV is not designed for a supportive, invitational, and ongoing recovery story.
Instead they want the drama, the confrontation, the badass story.
That culminates with someone storming out of the intervention but changing their mind just in time to fly off to rehab at the beach….. so this story line is reinforced to the general public.
Confrontation vs. Support
We tailor our interventions to the lowest common denominator. The narcissist needs to be confronted. But the majority with SUD need supported care.
And I understand why…. the punishing orientation is the only way to do treatment under our current reimbursement system.
Individualized approach to treatment is very hard to pull off when you have to pigeon hole people into groups. Group that meet 3x a week for 3 hours at a clip.
Or run a residential program for 50 plus people. You need people to “fall in line”. Or it’s chaos and mayhem.
Social Following Theory
Social following theory is the foundation of all group process and certainly the foundation for the residential experience.
You can’t have “social following” if you encourage individualism.
Social following requires group think. (This is why you will be put back into the remedial re-education group if you do not adequately “surrender”….).
This model allows for 10% of the folks in need to roll through the structure of treatment and for the reimbursement to follow.
Interestingly… the “confrontational, one size fits all, my way or the highway model”drives many potential patients away from services.
More “Hard Realities”
The tough love stuff runs many people off.
The language around treatment and recovery runs many off.
If a person in need tries some groups and they can’t fit in the box they don’t come back.
We tell people to go back out and “have more pain” then “come back when you want it”.
Sometimes we say this in subtle ways. Sometimes overt ways.
ALL OF THIS IS VERY CONVENIENT FOR THE PAYER. THE INSURANCE COMPANY. THEY DON’T HAVE TO CUT A CHECK IF THE PERSON DOES NOT SHOW UP. So 90% no show works very well for their bottom line.
Make the Addict Suffer
By the way. The “make the addict suffer” approach will also resonate with many families because they are so frustrated and angry with the person’s behavior.
And because they are uneducated on the details of addiction and recovery. And of course it resonates with the “law and order” elements of society.)
It’s a perfectly designed system that has evolved over the decades. The system will always produce the exact results it was designed to produce.
Favor Greenville – Innovation Saves Lives
FAVOR GREENVILLE has started a program in the hospital where we are working with those who “never surrendered”. Those who hit bottom and have just scraped along the bottom for decades.
They “just wouldn’t do what they were supposed to do”.
And after years and years of misuse they are now laying in a hospital bed.
Inpatient, for a wide variety of medical conditions the direct result of use. Alcohol mostly.
But other things as well. The costs are staggering. The hope has been beaten out of them. The healthcare system doesn’t know what to do.
Do you just let them die? Is that what we should do?
After all they “Didn’t want it”….. “They’re not willing” – Right?
The Installment Pain Plan
These are people with families. And with dreams. Human beings cut down way too early.
This is the result of “wait until they hit bottom” system we have built. Society should have been working on an alternative answer 20 years ago when many of these folks started their journey in and out of the hospital.
Their options should not have been limited to “groups and rehab” and “if you want it” recovery.
There are millions of people in America written off like this.
Slowly killing themselves on the installment plan. Because “they didn’t want it bad enough”…..
There is a Moral Imperative
And if you are sick enough to not care about the people. If you lack the humanity to see this as a moral issue then consider the financial implications of taking care of these people as they deal with these devastating conditions.
👊👊👊The system will always produce the exact results it was designed to produce.
But I hope you can clearly see.
It’s a system that desperately needs disrupted. There is a moral imperative to disrupt the system.