Things today are not quite like the “Good Old Days”, but there are still echoes in the air!
One of the main reasons people struggle with accepting addiction as a brain disease or disorder is because we act like such complete a**holes when we the disease is active. We do nasty things.
Sometimes its dramatic and very obvious like breaking the law, neglecting children, stealing from loved ones, abusing people.
These are the hardest situations to reconcile.
Very hard to have sympathy for someone who hurts a vulnerable person, those in the middle of active addiction.
Sometimes the behavior is more subtle; but still way outside the bounds of acceptable human interaction.
CONSEQUENCES & PUNISHMENT
Our behavior in active addiction leads to the desire for consequences and punishment to be levied.
In the obvious ways like jail, losing jobs, losing our kids, etc…
However, it has also contributed to the punishing nature of many treatment and recovery approaches.
Simply put, people want to extract a pound of flesh from the addicted person.
IT IS YOUR TURN TO SUFFER
The addicted person made many people suffer so now it’s their turn to suffer.
This is why the industry can basically do whatever it wants in terms of housing and services.
The general attitude is “those bastards are lucky they have a roof over their head. Who cares if they are working for $1.43 an hour at the sausage plant and living 7 people to a bedroom”.
LIARS, CHEATERS & THIEVES
Even the addicted individual himself joins in the punishment.
I’ve been in group situations where people just one upped each other on how completely horrible they were in active addiction.
We call ourselves “liars, cheaters and thieves”. We think that people being hard and being confrontational is a good thing.
I get it. I really do.
THEY JUST DON’T WANT IT
I understand how things have evolved and how we have progressed to this point.
A point where we can ignore 90% of people in need because they “haven’t hit bottom”. They “don’t want it”, RIGHT???
These concepts work for the everyday person on the street.
Interestingly, this framework also worked for families for years but that has changed quite a bit.
FAMILY SUPPORT BASED ON ALANON
Remember, historically, the foundation for family support was based on Alanon which was (and still is) mostly wives dealing with chronic alcoholism.
Again, it was very natural for these wives to be somewhat hardened and “done” with their husband.
I get that as well. My wife certainly fit that criteria.
The program that was developed would reflect that dynamic. This may be a challenging fit, however, for parents.
I will make the following observations however:
1 – NOT GOING TO WORK
It’s just not going to work.
We can not punish or arrest or lecture or confront or debate our way out of the addiction crisis.
If it was a behavioral issue perhaps that would work. But we all agree this is a brain disease… right?
2 – OTHER WAYS OUT THERE
There are other effective ways to talk about to people about their issues.
An alternative approach requires more effort and it requires creativity.
It requires a willingness to talk differently, lecture less and be open to new ideas.
It means dealing with challenging people with a great deal of patience.
3 – CONFRONT & BREAK THROUGH DENIAL
Eighteen years ago when I started as a clinician I was literally taught to “confront and break through denial”.
However, I blew that shit off early on. I could see right away the damage that did.
The “hot seat” for example.
People who facilitated that group had to have a willingness to re-traumatizing people. I refused to do it and they kept me anyway because I was absolutely freaking exceptional at my job.
Then I got promoted and changed all that bullshit. Good times.
THE GOOD OLD DAYS
I do believe the culture of confrontation is slowly changing. However, if you pay attention, you can still see and still hear the ongoing influence of the good old days.
BONUS RECOVERY CARTEL INTEL REPORT
Please check out this article from Los Angeles Magazines blog, April 23, 2018.
I am a master of manipulating a situation so that “everyone stays calm”. If I am not careful this will happen in all parts of my life. Work, family, friends. This is a learned behavior and a natural result of growing up in an alcoholic home. In a war-zone. If you upset the apple cart in my childhood home; all hell is going to break lose.
Classic: Don’t Talk…Don’t Feel…Don’t Trust….
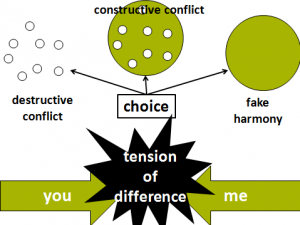
However, fake harmony is the enemy of setting boundaries. As I reflect on my life and the experiences I have had with families in the throes of a loved one’s addiction, I come to some pretty clear conclusions:
Setting boundaries is essentially the art of saying NO. Every boundary is essentially a form of saying NO. Sometimes very straight-forward:
“Can I borrow $100″… “NO you cannot”…
Sometimes it’s not as direct.
For example, a family member who drinks too much becoming verbally abusive when they drink… The boundary maybe you leave or it maybe they leave. But essentially it comes down to NO..
”You can’t treat me that way”…
So… what gets in the way of the boundary.
It’s not “what” to do. Most of the time we know that we should say NO. It’s “how” do we do it. Or maybe more accurately…why can we not do what is so obviously necessary and set this boundary?
1.)FEAR: We operate from fear of what is going to happen if we say no. We have scenarios that detail what is going to happen and we play them over in our mind. Fear controls us.
2.)JUST SAY YES: We plan on saying NO but in the moment, we allow the person to bully us into saying YES. They use intimidation, manipulation, and sometimes subtle techniques to keep us from saying NO. Example, give you the cold shoulder. Example, get you off task talking about other issues. Example, debate you to death. You give in just to shut the other person up and have some peace.
3.) PLEASE LOVE ME: We want the person to love us…or at least like us. So, we say YES as a way to not lose love and affection. In these cases, we tend to keep talking even after the boundary is set because we want the person to be happy about the boundary is set and life to be wonderful. They aren’t going to be happy. You just told them NO.
4.) I DID IT: Straight up guilt… We tell ourselves “it’s our fault”. The guilt clouds the rational decision making.
I’m a big fan of number 3… I need everyone I care about to like me and I need there to be peace in all my personal relationships. The reason being, I grew up in a home where unrest, discord, tension, resulted in really bad things. For me there is no in between.
Everyone is happy and everything is either really good…or the stuff is about to hit the fan.
In essence, I was always afraid of “destructive conflict” because I never knew there was “constructive conflict”. My response was to manage the situation and use my people skills to avoid direct confrontation. Of course, this approach has a short shelf life. It is unsustainable.
Constantly ignoring your own feelings does not change the reality of the situation.
How do you set boundaries in the face of these underlying issues. I would propose the following:
1.)For the fear based boundary challenges: There is a technique called “fear setting”. This is not for everyone because it can be a heavy duty emotional exercise. Fear setting involves getting in touch with the “worst case scenario” and trying to “sit in” the experience. Using guided imagery you can walk yourself through a mental exercise where the worst case scenario is played out. The idea being, if you can face this fear. You can set and maintain the boundary.
2.) For the “debater” and the “intimidator” challenges: The technique is called “hit and run”. Also structure the conversation. Make sure you have the conversation under conditions that naturally limit time for “discussion”.
Over the phone so you can employ the “I have to go now” technique. Or set the expectation at the beginning that you can only talk briefly. Be careful not to set the boundary talk in a circumstance where you can be held hostage. You don’t want to be a captive audience and enter in an extended debate concerning these issues.
3.)For the “we want them to love us” challenge: The technique is called “suffer in silence” and essentially boils down to this: learn to stop talking. How do you get comfortable with something that is initially uncomfortable? You “sit in” or “lean in” to the experience.
Try and be grateful for the opportunity to “learn from this discomfort”. You have to re-frame the experience in a way that is positive. If you don’t you will instinctively run from the uncomfortable feelings. Feelings will not kill you. Feelings will not physical harm you. Feelings will pass. Practice and keep track of improvement in this area.
Eventually you will become a boundary setting NINJA!
Like my beloved Melissa. She can drop the hammer and slice you up with a boundary and you don’t even know what hit you.
4.) How to handle guilt:
Here is a Rich Jones original method for addressing guilt.
It involves confronting the irrational thinking involved in your assessment of the situation. Journaling can be very useful. At the top of the page write out the boundary.
Example:“I just told Rich “no” to paying for his rent another month”.
Followed by: This makes me worthy of guilt because…. And let the words flow.
Get into a process of free association around this topic. Then put the journal down. Go for a 5-minute break and come back and read your reasons for feeling guilty. Let me know if the reasons are rational!!! This will condition your brain to confront the irrational thoughts associated with feeling of guilt.
Remember, setting boundaries is a skill. Or maybe more accurately, a habit. A habit is merely a behavior we engage in on a repeated basis. If you practice this skill you will get better and better at setting boundaries.
It may never be easy. But it will become manageable.
Boundaries is a word that gets bantered about all over the place in the recovery world. Actually it gets thrown around in all aspects of life. People devote extensive time to working on boundaries and setting limits within relationships. It is most certainly one of the key aspects of leading a healthy life. Without boundaries you can lose yourself and, in extreme cases, become involved in abusive relationships.
How do you “do” boundaries? What are the skills and guidelines for setting boundaries? Many times, a circular conversation ensues around setting boundaries:
Family member (FM): I don’t know what to do my kid just keeps smoking pot in his room and I have told him to stop.
Very Helpful Person (VHP): Well just set a boundary about smoking pot.
FM: How do I do that?
VHP: Just tell him. Stop smoking pot or there will be consequences.
FM: I tried that. He is still smoking.
VHP: That’s cause you didn’t set the boundary.
FM: What boundary?
VHP: The one about smoking pot.
FM: How do I do that?
VHP: Just tell him. If he doesn’t quit smoking pot there will be consequences.
FM: What kind of consequences?
VHP: Take his phone.
FM: I tried that. He just flipped out until I gave it back.
VHP: That’s cause you need to set boundaries about how he talks to you.
FM: What do you mean?
VHP: Tell him he can’t talk to you like that.
FM: He knows that. He does it anyway.
VHP: Well you need to get better boundaries… I heard they are having a sale at Walmart. Two for one. Let’s go.
Maybe I’m exaggerating just a bit. I am the king of hyperbole. However, the process of setting boundaries is much more involved than a simple declaration of intent. There are entire books dedicated to the concept. Maybe we can keep it simple by focusing on a variation of the classic saying: Say what you mean! Mean what you say! But don’t say it mean! How does this apply to addiction and family recovery.
Say what you mean!
“Saying what you mean” is about consistency between one’s thoughts and words. It is a plea to be honest, to truthfully represent one’s understanding, state or intent when describing it verbally (Runion). This is difficult for everyone. It gets especially challenging when addiction enters the picture.
Consistency between one’s thoughts and words presupposes that one has awareness of one’s thoughts. It has been said that the average human being has at least 77,000 thoughts per day and the overwhelming majority operate below conscious recognition. Under the best of circumstances we have difficulty staying in the present moment. Our behaviors and words are influenced by past experiences and future considerations. It is hard to have consistency when you aren’t even sure what you are thinking. It is as if life “just happens”.
Now add in addiction and all the chaos, drama, and fear associated with that reality. I would argue that a family member living through a loved one’s addiction experiences post traumatic stress disorder. Traumatic experiences are encoded and frozen in the information processing system of the brain making thought recognition even more difficult. At any given time family members will be triggered and re-experience previous events and situations.
How can you say what you mean when you aren’t even sure what you mean?
Therefore it is important to gain an understanding of “what you mean”. What is it that you want to see happen? What is the specific problem that you need to address? One of the ways helpers inadvertently confuse the family even further is by telling them “you need to work on yourself”. This muddies the water because many times the family actually wants to “help” their loved one. I’m hear to tell you. That is perfectly understandable.
After you work through “what can I do” family members will frequently come to the conclusion that they must change some of their behaviors. This is where the boundaries talk comes in. Some recommendations:
Identify “target” outcome-How do you want to be treated?
Remember the target outcome is about you not about the other person. Ask yourself: What do I need to be different in order for my life to improve? Try to avoid focusing on the behavior of the other person excepts as it relates to you. A quick example:
Johnny returns from rehab and is living at home with you. He’s 22 and not sure about going back to school or going to work. Johnny tends to go out late with his friends. He is 22…the night starts for him at 10 pm. You are 50. The night ends for you at 10 pm. Johnny tends to come in at 1 am. You are frequently up all night waiting for him to come home. Even though you aren’t sure he is using your anxiety and worry gets the best of you. The lack of sleep is starting to impact your life. You realize you can’t go to sleep until Johnny is “in for the night”.
At first glance the issue seems to be Johnny not coming in at a reasonable time. Your impulse may be to break off a speech about a curfew and coming in at reasonable hour. However, for a 22 year old 1 am is reasonable.
The real problem is your lack of sleep. So the target is: “I would like to get enough sleep” NOT a random curfew for Johnny.
This changes everything. Say what you mean in this case is translated as “I NEED TO GET A DECENT NIGHT SLEEP or you won’t be able to continue to live here. Something has to change about how late you stay out”. The details of this can actually be worked out with Johnny. Maybe this means he agrees to come in at midnight. Or maybe it means he agrees to spend the night with a positive friend rather than come home late.
Mean what you say!
“Meaning what you say” is usually about consistency between one’s words and subsequent related behavior or actions. This is where the rubber meets the road. Meaning what you say implies that you can carry through with what ever limit you set forth when you “say what you mean”.
The most important part of this process is thinking it through before you set the boundary and discuss the limitations and associated consequences. If you make statements that you cannot carry through on your authority is significantly undermined. It is better to say nothing at all than to make an empty threat. Of course, this is easier said than done. You need to develop ways of “pausing” before speaking on these subjects.
You also need to develop a team of people who can support in processing situations and exploring options. Parents for example, need to support one another in the decision making process. If there is disagreement around boundaries this will become a glaring problem when the boundaries are enforced. Sometimes a trusted coach or sponsor can help your family discuss these tough issues. Sometimes a therapist or counselor will be necessary. In some cases the parents will need to address deeper issues. The graphic below is meant to describe the importance of having crucial conversations regarding these underlying issues. Sometimes the “rules” and techniques (boundaries) need to wait until the foundation is shored up. For example, its hard to make sure everyone is on the same page regarding boundaries if mom thinks dad is “just not a good parent” and “does not want the best for the kid”. This will require clinical support to work through these complex issues.
In addition to parents, it is sometimes necessary to bring extended family into the discussion. Grandparents for example are intimately involved in many kid’s lives. Extended family members and friend have influence. They need to be on the same page with many of the boundaries that are set in these situations.
Furthermore, parents and extended family should discuss ways to give each other respite and support. Recovery is a process not an event. A marathon not a sprint.
Once the boundaries are agreed upon it is important to stay involved with your support system so that you can carry through over the long term.
Even more importantly, it is important to communicate these expectations clearly to your loved one. This is where the final part of the formula comes in.
But don’t say it mean!
Addiction is a beast. It can bring out the worst in all of us. The addicted individual will engage in outrageous self destructive behaviors. Stealing, lying and manipulating may become common place. If you aren’t careful your loved one will have you believing that 2 + 2= 8.
In turn this can bring out frustration in the family. Family members can lash out in anger and say things in aggressive ways. Impulsive statements about “throwing you out” become commonplace. Clear communication is going to take an effort. There is no easy way to maintain your cool in the face of an addition related crisis. However, here are some general guidelines:
VERY IMPORTANT: KNOW YOUR TRIGGER AREAS. ASK FOR HELP WITH YOUR BLIND SPOT.
Perhaps most importantly is recognition of your “hot buttons”. If you are going into a potentially conflict laden situation gaining awareness of what gets you fired up is very important. You may need to ask for feedback from you spouse or other family members in order to identify this. Many times these issues fall into our “blind pane”. However, identifying these potential trigger areas is vital to successful communication of the boundaries.
Don’t confront the person when they are under the influence. Wait until the next morning. Unless it is immediate crisis and person is danger to self or others in which case enact emergency services.
Rehearse the conversation.
Bring bullet points or a script. The addicted individual will try and get you off track and will bring up things unrelated to boundaries. Stay out of the weeds.
If the boundary involves outside forces (ie…the person needs to be evicted, the person needs commitment, etc…) make sure you have all the extraneous details worked out. Paperwork, phone calls to rehab, list of shelters. Bring this to the meeting. Again, having a family coach or a group to support you in this preparation can be helpful.
Have the conversation when you have energy and you are not already emotionally depleted.
I want to go on the record. This is all easier said than done and none of it is an exact science. Please become involved in local support groups and seek out professional assistance as you prepare for these conversations. Managing boundaries is hard enough. Addiction makes is downright overwhelming.