I guess there are only so many different ways to look at the addiction epidemic. Reminder—88,000 year die as the direct result of alcohol. 65,000 die from overdose. Over 150,000 dead. The worst public health crisis in American history and it’s been going on for decades.
WHICH ONE ARE YOU?
1) SHEEPLE: You don’t even notice it. American Idol is on.
2) SELF-RIGHTEOUS: You notice it but due to your own skeletons in the closet you project disdain onto those with substance use disorder (probably because you have your own unresolved porn addiction or food addiction or your mom/dad had substance use disorder etc…).
You say “they did it to themselves I don’t care what happens to these people”. Your suggested solution to this issue is to build more jails. OR start executing drug dealers and probably sprinkle a few drug users in there for good measure.
Note: these 2 groups are unreachable. Their opinion is not important but we must note they exist.
3) COMPASSIONATE BUT MISINFORMED: You notice the problem. You are not completely sure what to make of it. You may or may not be directly touched by it. Regardless, you have great compassion toward people dealing with this issue. You are seeking info and want to help. (Perhaps some of our policy makers fall into this category).
But you are probably getting much of your info from the wrong people. The system insiders who are gonna play out the same old narrative. OR The academic who wants to talk all research. OR The “governors commission on opioids”. etc….
YOU NEED TO LISTEN TO SOME ALTERNATIVE VOICES AND ASK YOURSELF: DO WE NEED MORE OF THE SOLUTION THAT HAS RESULTED IN 150,000 DEAD YEAR OVER YEAR. OR SHOULD WE TRY SOMETHING NEW.
4) STATUS QUO: You acknowledge the epidemic. You see it for what it is. You have genuine concern.
Perhaps this has been your life’s work. But you view the problem as a) under utilization of an otherwise relatively adequate and “functional system”.
In other words it’s not a system or provider problem it’s an “non compliant patient problem”. OR b) lack of access to an otherwise wonderful and working system. OR c) your business model is working quite well thank you. Rinse and repeat is good.
Your suggested solution probably involves more money for more of the same services. AND PERHAPS SOME TWEEKS TO THE EXISTING STRUCTURE. But fundamentally you think everything is okay on the “solution end” if people would just “do what they are told”.
NOTE: I don’t know what to say to you. 150,000 dead a year seems to be evidence of a MAJOR FUNDAMENTAL problem.
5) RADICAL CHANGE AND NEW SOLUTIONS: You are deeply troubled by the issue and it’s clear to you that the ship is sinking. You know something is fundamentally wrong and the solution involves something brand new.
You have no beef with old school approach, in theory, but you notice it doesn’t work for the overwhelming majority of those in need. You love the people working in the system but you hate the system itself.
You watch with tears in your eyes as addicted people and their families are exploited to pass legislation that props up existing practices. And you watch with growing anger as the CDC reports another increase in the death rate. You don’t want the existing system to go away altogether but you aren’t naive.
You know incremental additions or changes will make ZERO difference.
IF YOU FALL INTO THIS CATEGORY WE SUGGEST YOU CHECK OUT AUTONOMOUS INDEPENDENT RECOVERY SUPPORT SERVICES. THE MISSING PUZZLE PIECE.
WE NEED THE PEOPLE IN CATEGORY 3 TO MOVE TO CATEGORY 5.
✌✌✌CATEGORY 4 WILL BE A TOUGH SELL.
What other categories exist? What category are you in?
An interesting development is unfolding within the addiction treatment and recovery “industry”. An emerging emphasis on family recovery.
Treatment programs are promoting their “family recovery” support services and recovery organizations are also touting the merits of family involvement. The term “family recovery coach” is become more and more mainstream.
This is a positive step. However, I will go on the record. Family recovery support services go way beyond a workshop addressing detachment and enabling. Family recovery support services fall on a continuum. Any level of support is better than no level of support. But, let’s be clear. Not all family recovery support services are created equal.
Of course, I believe the Family Recovery Support Services we offer are top notch. FAVOR Greenville has provided over 15,000 hours of family recovery coaching in a wide variety of settings.
We have engaged over 8,000 family members in individualized family recovery services since 2013.
What We Have Learned
We have learned what works and what doesn’t. We have learned the best way to engage family members in the process. We have learned how to provide consistent and effective supervision and continuing education to maximize the performance of our family coaches.
There is the “theory” of family recovery coaching and then there is the practice of family recovery coaching. Our reference point is the actual practice backed by solid theoretical foundation.
We offer a family recovery group on Monday Nights at FAVOR Greenville that averages 50 plus participants.
We talk a lot about accepting and dealing with the fear associated with living with a loved one’s active addiction. I am struck with the devastating nature of this CHRONIC disease and the deep impact it has on family members. There is a stark reality; it seems we are never out of the woods where addiction is concerned.
“Families just want to see light at the end of the tunnel.” – Rich Jones
We hear consistent stories from family members and we have been able to identify themes of family recovery. We know that family recovery, just as the addicted person’s recovery, occurs in stages. A common issue is the lack of recognition of the individual family journey.
Family members are frequently pushed to make decisions to “detach” and to “kick him out” before they are ready to make such a move. They are told they are “enablers” and they are “going to love their kid to death”. Some of the people saying these things are misinformed. Some are dogmatic and hold tight to antiquated beliefs. Some just don’t know what else to say so they turn to clichés.
Tragically, some are motivated by filling beds and use fear to push the family toward an intervention.
They have been told they “are sick too” and they need to work on themselves. They are told they cannot do anything about their loved one’s disease and they should “focus on their own recovery”. Many of the families run from support when confronted in these ways.
Many times, families arrive to group in a confused and terrified state.
What do we say to these families?
First, it’s okay to try and figure out a way to help your loved one.
Maybe an intervention is in order. Maybe your loved one is willing but you can’t find a resource. Maybe your loved one is already doing some type of recovery and you want to know how to support him.
These are all legitimate questions Our group and individual sessions address these types of inquiries.
***Please see our family recovery page and our Recovery Cartel YouTube Channel. We have a plethora of video support and information available.
In addition, we would want these families to know there are ways to begin their own recovery process. If they are ready there are steps that can be taken. It’s counter-intuitive but rather than obsess on loved one’s welfare focus on your own recovery plan. Your family recovery can positively impact your loved one’s recovery.
There are some universal basic suggestions to follow:
1). Practice daily maintenance/daily routine.
Morning prayer; devotionals; reading recovery related literature; exercise; talking to healthy people. Most people focus on “book-end” prayer or meditation routines. Starting the day with silence and prayer can help with stress and centering an otherwise chaotic world. Ending the day with gratitude in the face of addiction can bring unforeseen peace and rewards. It takes discipline but the payoff is real.
2). Find a way to address the inevitable stress and anxiety that arises throughout the day.
You will find yourself obsessing on your loved one’s welfare. Worry will be an all-day reality. A suggested stress reducer: Tap into the “The Free Three”: get outside; laugh; listen to music.
3). Re-fire to Re-wire: continuously redirect worry and rumination.
For example, tell yourself, “Dear God please remove this thought…” If that is not your style focus on your own mantra. You need to address the rumination in the moment and consistently redirect your thinking over and over and over and over throughout the day.
4). Get clear on what you can do and what you can’t do…in terms of helping your loved one.
Having clarity that you have explored all options will make it more likely you can focus on yourself.
5). Have a crisis plan.
No one should be subject to physical, verbal abuse or threatening. Be willing to call 911. Get educated on the commitment process in your state. Get educated on the legal process and remember that the legal system can sometimes be your friend.
Please sign up for The Recovery Cartel emails and blog posts. Stay tuned to our channel and to our Family Group broadcasts. We are all in this together.
It is possible, actually it’s likely, that the delivery of addiction treatment and recovery services will change at a fundamental level. The acute care model, as it currently stands, will essentially go away at the private level. It may endure at the government/publicly funded level.
One macro-level reason—the attention on the opioid crisis has lead to evaluation of the industry for the first time in history. White middle class kids started to die and people in the general public started questioning practices.
We are at the very beginning of that “questioning” process. Watch as the anger grows.
There are so many questionable practices to question.
I’m talking 5 to 10 years from now. Not tomorrow.
Driven by reimbursement policy, emerging best practices, emphasis on value based care, population health, and the horrible results of destination rehab. Most treatment will be local. The end of the destination rehab is near..
Out of network insurance reimbursement continues to change and is becoming more and more unpredictable.
The days of throwing millions of dollars in billing against the wall and seeing what sticks are numbered.
Less and less is going to stick. (ACA was an illusion) Revenue cycle management more difficult.
This, along with “local” treatment emphasis, will lead to hundreds of centers shutting down. The big boys will survive. And some niche boutiques. But the Walmart rehab days are limited.
There will be a push for addiction treatment services to be delivered and managed primarily through healthcare organizations. This will become best practice and standard of care. Further limiting referrals to the “drug and alcohol clinic”….. this discussion is already occurring nationally.
Professional Recovery Support services will become funded through diverse methods. CMS and commercial insurance will jump in because the cost effectiveness of the service too hard to ignore. Money talks.
As the model grows and gains momentum and validity. Imitation will run rampant. More “providers” leave the treatment fold and go back to running nursing homes.
Treatment Centers will then attempt to provide Recovery Support Services rather than “clinical” services. Some will convert. Many will butcher it. This will further eliminate many of the instant experts and more programs will shut down.
Hospitals take over the primary deliver of addiction treatment and form partnerships with Recovery Support providers. This is consistent with the management of other chronic diseases (diabetes, asthma, heart health) and the culture of healthcare and infrastructure exists to support Recovery Support services.
The BUBBLE HAS BURST….
This happens in every industry. Fundamental disruption. Creative destruction.
Out of the dust and the rubble a new system will emerge and 10 to 15 years from now it will be the norm. Standard practice. The new system will become “just the way we do it”….
You heard it hear First….. it’s now documented.
#nostradamus | #theearthisround | #askblockbuster
✌✌✌SIDE NOTE…One Group that may avoid this process is government funded system. That system is a monopoly. Like public education it may be untouchable.
6 PRINCIPLES THAT WILL TRANSFORM THE RECOVERY WORLD
“Cartel–an arrangement between parties to promote a mutual interest or goal… “
I believe it will take a RADICAL reshuffling of the current treatment approach & public policy to make a dent in this crisis. I say this because all our efforts, so far, have fallen short as indicated by the astronomical increase in over-dose deaths. If it’s a disease the primary indicator of successful care would be keeping people alive. Right?
All that we have done to this point has been predicated on our pre-existing approach/philosophy. All our money and resources have been funneled through our pre-existing system of care.
It’s going to take a massive shake to transform and usher in change. Our institutions will double down on current practices. Because that is what institutions do. They exist to sustain themselves. It’s a sociological fact.
The change could come via the free market. If treatment providers saw the wisdom of a new business model. However, that would only happen if current business dried up. “If it’s not broke don’t fix it”…. seems to be the prevailing philosophy. And I don’t see it drying up soon. Too deep a problem. Too much demand. Plus 70% repeat business makes the model self-sustaining.
The solution will come via “outsiders” AND NON-CONFORMISTS. Independent thinkers, people from other industries, progressive healthcare providers, and risk takers. Partnerships that, on paper, make little sense but in practice lead to transformational ideas.
THESE PARTNERSHIPS WILL PRODUCE RADICAL IDEAS. People will actively push back on the ideas. When that happens, it indicates that the proposed idea is probably the right type of idea…bureaucratic objection especially, is a litmus test for a great idea. Almost as promising as when a treatment provider tells you “that’s not the way we do it”…. then you are on the right track.
It’s going to take a cartel…A RECOVERY cartel. Like any good cartel we need to have our organizing principles and our mutual goals… From my perspective the CARTEL holds the following principles near and dear.
Within the CARTEL we embrace the concept of “keep coming back”. For us, this is not just a cliché or a theoretical ideal. For us, it is the measure of our success and the single most important aspect of the recovery process. We know that people who stay engaged in a recovery process, regardless of the specific pathway, tend to get better. Even if you struggle along the way your life starts to improve. Even if you “mess up” and use, things begin to get better. Furthermore, we believe that the vast majority of people that continue to work a recovery program do eventually sustain long term recovery.
On a very practical level this means we will never preach to you or judge you. It means that we are all on equal footing in terms of our recovery. It means there is no hierarchy of recovery or right or wrong way to do recovery. We don’t count days. We don’t prescribe specific pathways. We just want to see your life improve. We just want to see families get put back together. We will meet you where you are in this process. If you are still using our goal is to help you figure out next steps and how this behavior fits in with YOUR personal values. Not ours. We have no agenda other than your welfare.
We believe substance misuse is a healthcare issue. We offer you a place to discuss it as a healthcare issue. It is not a moral failing. If you are struggling with substances you probably have considered stopping. You may have tried before. We believe we can provide you with new information, supportive coaching and unconditional positive regard.
Our core recovery principles include the following:
1. You are in recovery if you say you are in recovery.
Admittedly this philosophy is NOT exclusive to the CARTEL. Many other recovery community organization have adopted this perspective. I have been in situations where the definition of recovery has been a hot topic of debate. I have been in situations where people have contested the merits of the term “in recovery” versus the term “recovered”. I have little tolerance for such things.
Entering into recovery is a difficult process. If we make people stand at the threshold and question if they “qualify” it is only going to drive people away. Therefore, for our purposes remember…you decide if you are in recovery. No need to fill out an application or get your passport renewed. You’re in.
We hope to assist you in the journey and we know that recovery is process not an event. If we offer advice and support it is in the spirit of guidance and it comes with unconditional positive regard. We stand in radical non-judgment of your journey. However, we will tell you if your ship is sinking. We will just do it in a very loving and caring manner. No shame. No punishment. No judgement.
We want to welcome you to recovery, regardless of how you define recovery!
Recovery is NOT a contest…
2. There are multiple pathways to recovery.
Again, this may not be earth shattering. As a matter of fact I hope people read this and say “of course there are multiple pathways. My fear is, there are many who believe that there are only specific ways to recover and any effort outside of that framework is futile, inferior and doomed for failure. I used to think that way. What a horrible outlook on recovery that was.
“Rather we shall reflect that the roads to recovery are many.” – Bill Wilson Co-Founder, Alcoholics Anonymous
People find recovery through countless avenues. Research indicates that the majority of people with a diagnosable substance use disorder will recovery via a process of “natural” recovery. In other words, they will find ways to eliminate their substance abuse and live a productive life without formal intervention and formal “recovery programs”.
I do not dispute this research. However, I have concerns with waiting for people to “figure it out”. In this age of overdose, we need to be very aggressive, assertive and effective in promoting recovery. That said, the key part of the message needs to be multiple pathways exist and you can invent your own pathway. We just believe that you can get that done more effectively if you have a coach or a mentor to help you figure that out.
Recoveryism is a term that has been used to describe the phenomenon that exists where people hold the position that their personal path of recovery is the “best path of recovery”. Actually, many believe that their personal pathway of recovery is the ONLY pathway of recovery.
This is a most dangerous form of tribalism. Can you imagine how many people have been alienated or chased away via such attitudes? There is no legitimate place for this in the recovery world and certainly should be ZERO tolerance for this in the professional community.
3. You should not be required to “quit” prior to becoming involved in a professional program. The person who is “not sure” what they want to do with substance use, has a right to, support, coaching, and direction.
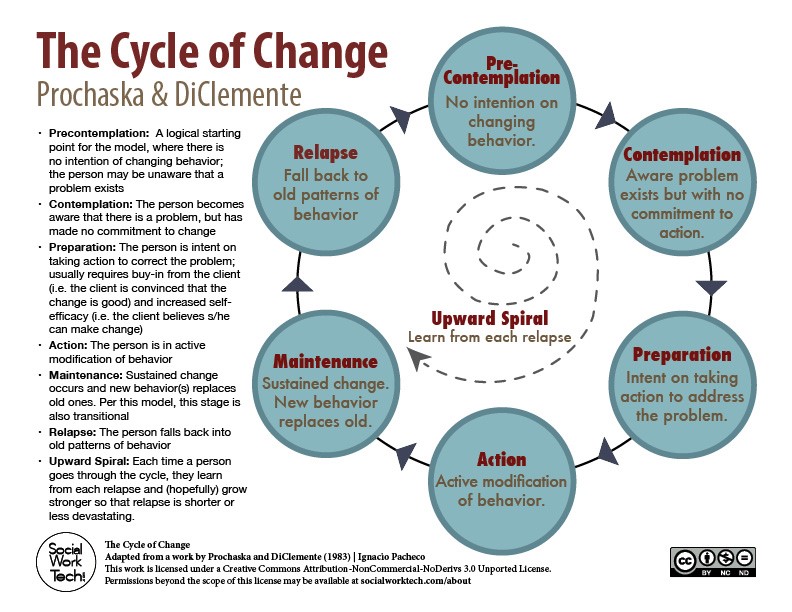
Change happens across a predictable and universal process. The stages of change have been well researched and validated over and over. They apply to anyone making a behavioral change including someone dealing with a substance use disorder.
Many people struggle with commitment to change and a constant process of “thinking about” change (ie. Contemplation stage). This is completely natural.
Most programs require “willingness” and will only work with the person in the action stage of change. We believe, instead, that working with a person in contemplation is just as important as working with the person in preparation or action.
We also believe that many people in contemplation will move to preparation and action if they have people to talk to about the issue. Processing information about the change moves the person through the change process. Isolation does not.
Therefore, we would love to see you even if you are not sure you want to quit. Even if you are not sure you are an addict. Even if you want to come to just get the heat off for a little while. We will help you get the most out of your experience.
4. We believe family recovery support is also a primary part of the process.
Family recovery stands on its own merit and should be available regardless of the status of the addicted loved one. Some type of recovery plan is essential for all family members. We know that family members can benefit and experience improved mental health, reduced stress and ostensibly better overall physical health. Therefore, the primary purpose of family recovery is improved health and welfare of the in and of itself.
However, we have observed an interesting phenomenon. When the family takes “care of itself” the addict frequently follows suit. This has been validated by a wide variety of resources. ARISE intervention model teaches this very philosophy. It was in my ARISE certification training that I first heard the statistic “1 family member is as powerful as 8 professionals”. Additional studies have been done on the impact of the family. Behavioral couples therapy for example has been shown to deliver around 66% success in getting the addicted individual into services.
Very important: Tough Love is an oxymoron. YOU NEED TO FOCUS ON APPROPRIATE EXPRESSION OF LOVE. NOT TOUGH LOVE. Sometimes, setting limits and boundaries is the appropriate expression of love.
We do not believe in complete disengagement. Many things you hear about family role in recovery are dangerous.
WE HOPE TO DISPEL THESE MYTHS.
5. We believe that recovery is a process not an event
We know that, statistically speaking, it takes on average 4 or 5 genuine attempts at recovery before “it sticks”. This isn’t to say relapse is a necessity. It is not. However, relapse is nothing to be ashamed of and should be met with loving compassion. There is a need to make “returning to recovery” as easy as possible.
We also believe that professional services that specialize in re-engagement are essential to the continuum. There is a glaring hole in our professional service structure and we need to provide long term support. We need to re-vamp our system to support long term, chronic disease management rather than episodic acute care.
6. And finally…we believe RECOVERY will bitch slap addiction if we allow it to.
If we come out of the shadows and conduct ourselves as responsible members of society the community will embrace us. If family members become open about their struggles the community will embrace them. There is power in numbers.
However, our efforts in this area have been set back by “advocates” who reinforce the stigma when they speak for recovery. Much work has been done on messaging and identifying the most effective way to carry the message. Market studies have been done. Focus groups have been conducted. There is productive way to share the message of recovery and there is a counter-productive way to carry the recovery message.
A public lead meeting or online speaker meeting is not the way to promote recovery. This type of spectacle works for those already in recovery. However, we are not trying to preach to the choir. We are trying to reach the masses. If the goal is true advocacy then please adopt some type of intentional recovery messaging.
If the goal is to fill your treatment center than keep doing what you are doing.
However, in the interest of “rigorous honesty” please give up the word advocate.