From the CASA Columbia “Analysis of the National Household Survey on Drug Use and Health”.
Please take a moment and cogitate on the picture in this post.
Observe if you will the 2 “poles” of the continuum.
In theory we address the entire continuum of substance use; but does our practice/approach match the diversity and stages of substance misuse? Of course not.
In American society we approach substance misuse primarily in the following 2 ways:
“Just Say No! Don’t Do Drugs” (focusing on the 12.7% “not using”). These are our prevention programs.
“Wait Until You Hit Bottom”; admit you are an alcoholic or an addict and come to treatment (focusing on the 15.9% “addicted”).
This is our reality. Substance misuse is not discussed until IT HAS TO BE DISCUSSED. Until it cannot be ignored.
And even then we do a horrible job connecting to that 15.9%.
From the CASA Columbia Addiction Medicine Report:
While about seven out of 10 people with hypertension, major depression or diabetes get treatment for their medical conditions, only about one in 10 people with addiction involving alcohol or drugs other than nicotine do, leaving a treatment gap of 20.7 million individuals. The proportion of individuals in need of addiction treatment who actually receive it has changed little since 2002, when 9.8 percent of those in need received treatment.
Failed at Engagement
IT HASN’T CHANGED SINCE 2002. 16 YEARS.
I would say that indicates we have failed at engagement.
If we can start touching the people who are in the non-risky and risky categories we can make a difference.
But they are NOT going to come to your clinic.
They are not going to listen to the “Just Say No” presentation at school.
If they are in the risky category the “documentary on addiction” is not going impact them.
They are not going to go to a meeting and admit powerlessness.
Quite frankly, meetings are NOT designed for the “risky user”; they are designed for the “real alcoholic/addict”.
They are NOT going to come to an intensive outpatient program unless they have to, i.e. DUI, and then they are going to go through the motions.
This is What We Need
Information, non-judgmental information, that does not involve a diagnosis.
That does not involve a prescriptive “program”.
Does not require “admission” to a certain type of problem.
This is what we need. Engaging information. Professionally delivered.
With a nod toward healthcare rather than a nod toward rehab.
The word recovery may even be problematic for the “risky user”category. They just aren’t there yet.
Carpet Bomb with Information & Connection
If we carpet bomb the country with information and connection at a “stage appropriate” level, I believe that will lead to more people in the “addiction”‘ category seeking treatment.
If we “touch” people along the way as they progress toward addiction they will be more likely to seek help once they do cross that line. OR even before they cross that line.
The challenge is doing so at a “stage” appropriate level.
Engaging Content and Engaging People
We can’t talk to the public the same way we talk to one another.
This goes way beyond using the term “substance use disorder” versus the term “addiction”.
Avoiding the term “substance abuse” is not going to win the day in this regard.
Engaging content and engaging people talking about health and wellness will make more of an impact.
Almost Impossible
“Identification” is hard enough for a person who has crossed that line into “addiction”.
It will be almost impossible for the “risky user”.
Unfortunately many of these “risky users” are being sent to rehabs that were designed for the “addicted” person.
Causing more harm than good?
Embrace Harm Reduction
This is also going to require that professional providers embrace a harm reduction point of view.
NOT in terms of M.A.T. or needle exchange etc… but in terms of reduction in use; less dangerous use etc…
Increasing community tenure. Getting away from knee jerk referrals to inpatient rehab.
Many of you are cringing while reading this.
Noble and Important Work
I love everyone who works in this field. Y’all are doing noble and important work.
But the logic of my argument is beyond reproach. Don’t kill the messenger.
If we are ever going to slow the rampage of addiction we will need to implement these type of comprehensive interventions.
Emphasizing quality of life and health/wellness over “recovery”.
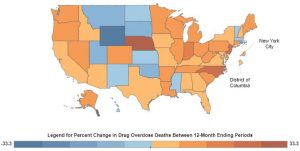
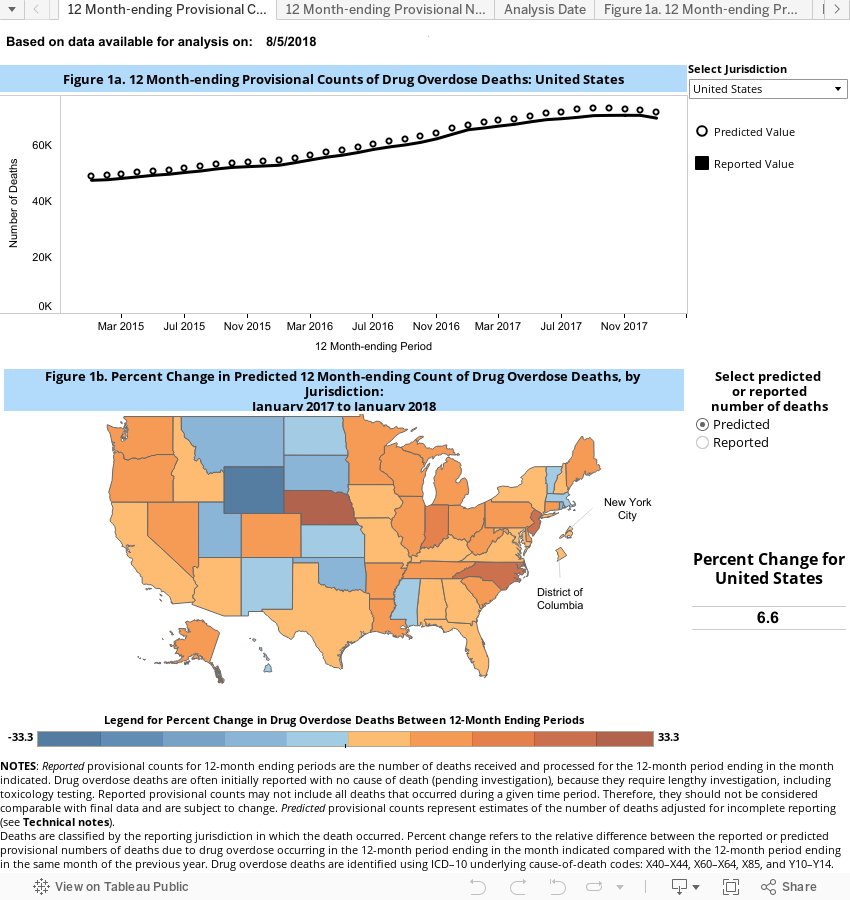
Horrible, bleak new estimates from the “Centers For Disease Control and Prevention” on overdoses – 72,000 in 2017.
“Drug overdoses killed about 72,000 Americans last year, a record number that reflects a rise of around 10 percent, according to new preliminary estimates from the Centers for Disease Control. The death toll is higher than the peak yearly death totals from H.I.V., car crashes or gun deaths.” – New York Times
If you read the complete article you will also see that “…there are also encouraging signs from states that have prioritized public health campaigns and addiction treatment”. The 2018 numbers are trending down in many parts of the country and the “rate of increase” is slowing overall.
However, 72,000 overdose deaths is staggering.
The New Normal
Unprecedented and hard to wrap your mind around that reality.
Furthermore, we know this is an “addiction epidemic” not an overdose epidemic. As we have discussed before; add in suicide rates and untreated mental health.
Record setting anxiety among young people. Are we still alarmed or are we numb?
Will these results become the new normal?
The response you see from the industry is a doubling down on standard operating procedure. Countless pleas for “more treatment and longer stays”. Countless pleas to the addicted individuals to “call now for help; save yourself”.
The answer to this crisis is not to simply keep shouting “come get help”…
OF COURSE WE WANT YOU TO GO GET HELP. OF COURSE WE WANT YOU TO GO TO A QUALITY TREATMENT PROGRAM. DO IT…GET HELP TODAY. CALL NOW!!!!!!!!!!!!!
Only 10%
But we know only about 10% of people will actually do so.
Are people still thinking that this statistic is a lie?
Do they think the federal government just makes that up?
Do people think that addicted people will all the sudden wake up and go get help because of a Facebook ad or television commercial?
All the sudden the unwilling are going to become willing?
Crossroad as a Nation
We are at a crossroad as a country…a crossroad as a society.
This is not unprecedented. This happens in the course of human evolution. It is not 1972. Things change.
When “rehab” was invented there was no internet, no cell phones, no fentanyl, no 18 year old heroin addicts, no K-2 spice, no kratom, no legal weed, no social media….
I mean, it is insane that the basic procedure and response to this issue remains unchanged.
Basic Procedure
Tell people they need help
Tell families not to enable
Wait until they hit bottom
Get them to go to treatment
Get them to go to 90 meetings in 90 days.
Watch them live happily ever after.
This will work if you work it… but what if you don’t?
Holy Cow…. It appears we are going to ride this bus off the cliff.
Addiction is Not a Disease – Really?
Overall Americans don’t think addiction is a disease.
We don’t treat it as a disease. We use the “disease of addiction” as a source of entertainment; TV shows; social media; etc….
We follow addicted people with cameras and document their use.
Document their self destruction and ugly behavior. We turn them into a sideshow.
Our policies do not reflect addiction as a disease. Imagine being an everyday uninformed citizen and coming across your average recovery feed or reality TV show?
Imagine the perception that person comes away with? Those of us in recovery may love to hear what is was like, what happened and what its like now…
But your average PTA member recoils at the “I was living in a dumpster behind Taco Bell” type details.
Addiction and recovery is becoming a circus freak show. Come watch the addicts put themselves on display. Good God.
A Need For Disruption
This industry is in desperate need of disruption.
But change in healthcare is difficult for many reasons and change in the behavioral healthcare space is even more difficult because of the “mysterious” process of getting better and the blurred lines between personal and professional experience.
Perhaps the most significant barrier is the “you’re gonna kill people barrier“.
If you try to do something radically different in this domain people push down the innovation by stating “that’s gonna hurt people; you’re gonna get people killed“.
As if people aren’t already dying?
Disruption implies the creation of something completely new.
Invention vs. innovation. Invention is creating something new. Innovation is tweaking the existing process.
ONCE MORE: TREATMENT WORKS IF YOU GO AND YOU ARE WILLING AND YOU “WORK IT”.
SO CALL NOW… GO GET HELP.
But this is way beyond that willing person… Sorry to be such a buzzkill…
Over the past few decades, practitioners and researchers increasingly have recognized the link between substance abuse and mental disorders. Some studies suggest co-occurring disorders are present in up to 60% of addiction treatment admits.
Defined as the presence of at least one substance use disorder and at least one axis 1 mental health diagnosis or axis 2 personality disorder. Some states have aggressively pushed COD services.
Clinical credentials reflect this commitment to COD services—for example:
I am a Certified Co-Occurring Disorders Professional from my days in Pennsylvania.
Treatment Improvement Protocol
There is also a SAMHSA guide called TIP 42 (Treatment Improvement Protocol) that serves as guidelines for COD services.
When it came out in 2010 (?) there were also TIP 42 trainer the trainer courses.
I am a Certified TIP 42 trainer (talk about an obscure credential).
Facilities in PA could also become accredited as COD INTEGRATED (the highest standard) or COD COMPETENT clinical facilities.
The hope was that COD services would become the norm. This “movement” has lost much of its momentum.
I am of the opinion that the mismanagement of COD issues is the second most dangerous issue facing individuals and families seeking help.
Behind only straight up body brokering.
The 4 Quadrants
COD comes in many different manifestations
Q1—Quadrant 1: LOW Mental Health/Low Substance Use Disorder Q2—Quadrant 2: LOW Mental Health/High Substance Use Disorder Q3—Quadrant 3: High Mental Health/Low Substance Use Disorder Q4—Quadrant 2: High Mental Health/High Substance Use Disorder
1-800 CALL-CENTER
The problem is when someone calls your average addiction treatment “helpline” or “treatment line” hey will almost automatically be pushed toward rehab. (They almost diagnose the problem with little or no MH training or education.)
You hear it all the time.
A mantra of get them into detox, rehab, long term residential care.
There may be a sense that having a psychiatrist on staff will take care of the possibility of a COD.
That’s woefully inadequate.
If it is a Q1 or Q2 issue it would be no harm no foul. Much of that can be handled.
Very Specialized Care
If it’s a Q4 issue you need very specialized care. The most troubling is a Q3 (high Mh/low SUD).
Many times a family member will call an addiction treatment program with a Q3 situation because it looks like SUD may be the problem.
When in fact it is a symptom of the primary mental health issue.
A great example of this is breakthrough mania associated with bipolar type 1.
The mania frequently involves a wide array of risky, impulsive, dangerous behaviors that could include out of control drug or alcohol use.
More Harm Than Good
And it is possible that taking a person with true bipolar type 1 and plugging them into your standard addiction treatment setting results in more harm than good.
Again….having a psychiatrist on staff does not mean it’s competent the effectively work with co-occurring Disorders.
Require Competency
To be COD competent require competency in skills training, working with families and case-management directly related to the mental health issue.
Telling a Quadrant 3 client that their aftercare plan is attending an intensive out-patient, and go to 90 meetings in 90 days, is….. well problematic at best.
Be Extraordinarily Careful
YOU OR YOUR LOVED ONE IS HIGH MH (Q3 or Q4) you are better off in a MH primary facility if there is no COD competent program.
I fully understand that access to integrated COD and competent COD facilities is lacking.
And many people can’t afford top notch COD care. In those cases you may need to piece together a solution.
Please understand if you call one of the “get help now” phone lines you will be steered to addiction treatment. If Q3 or Q4 is your loved one’s reality you must be extraordinarily careful.
✌️✌️✌️It will be necessary, in my humble opinion, to engage technology fully in addressing substance use disorder and mental health.
Our front-line, first response to these issue can not continue to be waiting for willing people to go to rehab or waiting for willing people to wake up and see a psychiatrist/therapist.
These traditional providers could could continue to play a role in a brave new behavioral health world. There will no doubt continue to be some willing folks “show up” and adhere to “treatment plans” (10% in SUD; tops 30% in MH)
However, full engagement of technology will be necessary to stem the tide of overdose, alcohol related deaths, suicides etc… (Deaths of despair).
Artificial Intelligence
Society uses machine learning and artificial intelligence in every aspect of life.
Data collection and profiling leads to internet platforms that anticipate your needs and send you a pro-active advertisement. It’s as if “they” are reading our minds.
I’m not saying this is a good thing. I think the ethics of “big data” is yet to be hammered out. But I am saying it’s noteworthy.
Could technology be used to a) engage more people in need; tap into this data; profile and send pro-active messages of support. Maybe even intervene.
There are companies already exploring this possibility. b) provide base level coaching?
I know you are going to flip out and say “counseling can only be done face to face; counseling requires a human interaction”.
Identify Common Themes
Here’s my response. Yes; there are issues that must be addressed through a traditional setting. More serious, deeper issues. Trauma for example. But after 18 years of mental health and addiction work I could identify some common “lower level” themes that could be addressed.
Furthermore, people are NOT showing up to address these base level emotional issues because it hasn’t “gotten bad enough yet”. Easy access and engaging technology would put a dent into these unaddressed issues. c) as stated above identify at risk people and pro-actively intervene.
Big Brother Type Stuff
There are many objections that can be raised. There are many reasons not to do this. This sounds creepy. It sounds like big brother type stuff. But the big brother type stuff is already happening.
The difference is they are using the data to sell you a $3 t-shirt for $75.00. They are using the technology to successfully drive consumerism. Could technology be used for noble reasons.
To solve the number one public health issues facing America; Untreated mental health and substance misuse.
Time and Money
Another barrier is cost. Full engagement of technology requires massive investment in time and money. It’s not something you throw together on the side and it goes way beyond a monitoring system/app.
✌️✌️✌️The Demi Lovato overdose has really brought out a bunch of “experts” to tell us the ins and outs of addiction. Who are the gatekeepers that arrange this stuff? How do they pick the “expert”… have any of them actually worked with a person with SUD or with families?
It may not matter because the media is looking for a cliche and a sound bite. And those are easy to come up with. The “expert” can deliver that.
But is all this attention and noise thrown Demi Lovato’s way good for her? Or good for society? I guess it’s good for the “experts”.
The Circus Has Come To Town
It a freaking circus. My home page is Yahoo News and here are a couple of stories that popped up over the last few days (I’m paraphrasing)
1) Demi Lovato overdosed because she bought into the “moderation” lie. With some idiot proclaiming with authority the abstinence only dogma. Like they know everything about Demi Lovato and why she overdosed.
2) Demi Lovato overdosed because she “gave up”… well damn…. they seem to have figured that out from some song she recorded about 6 months ago….geniuses.
3) Demi Lovato overdosed because of a “negative body image”…..HOLY MOLY! There must be Jedi therapists out there who can evaluate people from afar and make precision diagnosis.
Y’all depress me. You aren’t experts. You don’t know anything about Demi Lovato. Y’all should turn down the interview. It’s not a sideshow. It’s someone’s life. And it’s damaging to all people seeking recovery.
When a celebrity has a recurrence of cancer is it publicly announced and scrutinized? Do they evaluate “where it went wrong” what the celebrity patient did wrong leading to the recurrence?
This is par for the course for the media. But the “recovery experts” should not contribute. It’s not good. It’s not “awareness”. This is not “advocacy”. It’s a circus.
When Netflix first started steaming videos Blockbuster laughed at such an idea.
They were certain that people were going to continue making their weekly trips to the video rental stores. They couldn’t imagine a brand new way to do home video.
Well, Netflix could. And then they invented this new way.
And Blockbuster was left out in the cold. We need a Netflix of recovery.
A New Idea
What follows is an example of a new idea to solve our current crisis.
To address DEATHS OF DESPAIR. Annually: 65,000 overdoses. 45,000 suicides. 88,000 alcohol related deaths. Record high anxiety. Record high levels of “loneliness”. Cultural rot.
Nothing Changes if Nothing Changes
Let’s start with a basic principle: Nothing changes if nothing changes. We can agree on that.
Unless we act decisively these trends will continue and they will escalate.
Can we also agree that reversing these trends will require innovation and invention? By the way, if you think everything is fine the way it is and these results are acceptable stop reading this.
The Federal Government Will Need to Act
Second principle: the federal government will need to act as venture capitalist and put up the initial money for the payout.
And/Or Mark Zuckerberg or Bill Gates or these other larger national foundations.
If it works in a couple of pilot programs perhaps permanent reallocation of the dollars could follow?
Insurance and criminal justice and behavioral healthcare funding gets reallocated because the results are so staggeringly good. Back end monetization is the only flaw in this plan.
I know the current structure would push back hard against any change.
From a sociological perspective it is very realistic to create a matrix of community behavioral health severity. A rating scale on how bad it is in any given county in America.
Many academics would jump all over this. Especially if it was tied to transformation.
Run some analytics on insurance claims, mortality, incarceration related to substance misuse, emergency room utilization, and many other social determinants. This becomes the “score”. This is not hard to do….
Then put out request for proposal to “fix” this problem.
5 Year Study With Mass Payouts
Make it a five year study. Set the parameters for the target metrics. And offer a MASSIVE INCENTIVE. A MASSIVE PAYOUT AT THE END OF 5 YEARS if these targets are hit.
Tell the “companies” that want to get in on this: they need to figure out how to bring the score down.
Don’t prescribe the protocols. Let them invent the protocols. This idea would bring the power of free market enterprise to bear on this issue.
You would see the power of entrepreneurship unleashed on our crisis of despair.
It would be best if this was open to any vendor. Not limited to the existing healthcare or treatment providers. As a matter of fact it would only work if there was low barrier to entry for any and all vendors.
RJ Corp. – Traders of Knowledge!
I personally would love to get in on something like this. I will start the company tomorrow.
The current behavioral health system makes its money and maintains its power and prominence from the same broken system we are proposing they fix?
Do you see the lack of logic in expecting innovation to arise out of this arrangement?
Do we actually think people in the existing system and structure are going to work to make their own model obsolete?
A Really Cool App
Adding a new trauma therapist to the team or increasing access to medication assisted treatment or hiring a mental health counselor for schools is NOT INNOVATION.
Even a really cool app to track progress.
It’s all the recycling of the same service and approach. More of the same. For example, the app is just a new way for “willing people” to journal.
Unless we change the incentives we stand no chance of changing the outcomes. ( Basic Principle #1)
It will take appropriate compensation to attract talented people and creative thinkers from outside the Recovery Bubble.
It would be fantastic. The status quo would stand by and watch…. thinking it silly and a “fad”…. then they wake up one day and realize the world has changed and they better cancel this year’s golf tournament and victory lap at that posh resort….
We know that in any given year, only 10% of those with an addiction issue receive any type of assistance or help.
As it currently stands, we are having difficulty meeting the needs of the 10% that do show up. Can you imagine if the other 90% showed up? It would be an absolutely unmanageable situation.
We know we are in need of some serious changes. We know we need real innovation.
What do we know about innovation in general?
When you learn about innovation there are some clear factors that are universal across all industries.
Two of the most pronounced issues associated with innovation are business models and governing beliefs.
Business model is straightforward. It’s the “how we do what we do to make enough money to keep doing what we do”. Governing beliefs can be overtly stated, but many times, these are the unspoken rules and perspectives that drive the industry.
Rotman Management Magazine states that “every industry has it’s governing beliefs”.
These beliefs tend to drive decisions and many times will be a barrier to innovation. According to Rotman no industry is beyond developing dysfunctional governing beliefs.
Let’s explore these factors a little closer:
You cannot innovate within an existing “business model”.
All you can do is incremental improvement. The existing traditions, norms, culture, practices, ingrained thinking will always “rub off” the innovation.
They will take the square peg and shave it down until it fits into a round hole.
For example, the addiction conferences where they talk about an “app” to monitor the behavior of an already engaged and willing client…that’s not innovation. That’s an upgrade.
Like adding remote start to your Toyota Camry. It’s cool. But not innovation. All the fundamentals remain the same.
In all industries the business model is driven by governing beliefs:
Therefore, in order to have innovation we must change governing beliefs. We must have a paradigm shift. The prevailing governing beliefs of addiction treatment/recovery services currently are:
A person must experience sufficient consequences and “pain” in his life in order to become “willing” to “enter treatment”.
If the person does not succeed in treatment (or post treatment) it is generally his fault. Mainly: “he wasn’t ready”.
Multiple trips to rehab and to treatment is good for business. There is no incentive to keep people out of rehab. There is no incentive to support after-care in anything that resembles a substantive way.
Generally speaking there is one way to recover and it involves completion of treatment followed by attendance to community-based meetings.
The real money is made in the residential space and the main way we fill beds is either business development staff (the light) and/or SEO ; pay per click; patient brokering; make me throw up marketing strategies (the dark).
Nothing new. Just more convenient.
Innovation, to this point, has taken place within the context of these fundamental beliefs:
An example of this is the explosion of “recovery apps” that pre-suppose “a willing and engaged” participant.
The participant “inputs data” and they tracks their own progress. The participant receives feedback and direction and is receptive to all that.
This app follows the governing beliefs of the industry. Namely, a participant must be actively engaged, motivated and willing to become involved. Nothing new. Just more convenient.
Rehab is the Answer. Why?
Another example can be found in all the “family advocacy/recovery programs” that are primarily focused on “getting people into inpatient treatment”.
They adhere to the governing belief that “rehab is the answer”. Why?
What about the foundations and scholarship funds dedicated only to “beds”. Why?
What about the government over-emphasis on dollars for treatment and the outright disregard for recovery support services. Why?
Does anyone ever take a moment and actually question “Why are we doing it this way”?
Especially in light of the results we are getting!
Every other industry is in a constant state of creative destruction and innovation. The advancement of the human race is built on innovation.
A Complete 180
It stands to reason then, that in order to embrace true innovation, we would need to turn the paradigm 180 degrees:
A person DOES NOT have to “want it” in order to get better. Indeed, most people are not internally motivated when they enter recovery. Waiting for “bottom” is illogical and inhumane.
A PRIMARY RESPONSIBILITY OF TREATMENT/RECOVERY/HEALTHCARE is to find and engage these people before they get worse.
If a person does not succeed in treatment (or post treatment) the primary responsibility lays at the feet of the provider (of course there will be exceptions to this rule).
Providers should make more money if the person is successful post rehab/treatment. Multiple trips to treatment is a sign of a flawed program.
Invent brand new ways to recover and allow the participant to guide that process.
Residential treatment should be an afterthought as the real work is done in the community and reimbursement should reflect this reality. A de-emphasis on “filling rehab beds” would be a game changer. We could then spend our time on finding solutions.
The most obvious questions are:
Why is innovative thinking so rare in the addiction treatment space?
Why is it so difficult to challenge our governing beliefs?
The simple answer is the PLAYERS, FUNDING AND REGULATIONS makes the treatment industry landscape infertile ground, in terms of much needed innovation.
NOTE: In order to understand the barriers to innovative thinking in addiction treatment we will use macro-level healthcare innovation as a context.
Harvard Business Review
In the article “Why Innovation in Health Care Is So Hard” Harvard Business Review identified 6 “forces” affecting innovation. Let’s will look at some of these areas and see how they apply to addiction treatment.
THE PLAYERS –
As HBR states:
“The health care sector has many stakeholders, each with an agenda. For example, hospitals and doctors sometimes blame technology-driven product innovators for the health care system’s high costs.
Medical specialists wage turf warfare for control of patient services, and insurers battle medical service and technology providers over which treatments and payments are acceptable.
Inpatient hospitals and outpatient care providers vie for patients, while chains and independent organizations spar over market influence.
Nonprofit, for-profit, and publicly funded institutions quarrel over their respective roles and rights. Patient advocates seek influence with policy makers and politicians, who may have a different agenda altogether—namely, seeking fame and public adulation through their decisions or votes”.
THE HOLY COW!!!
Tell me this doesn’t apply to the addiction treatment and recovery space?
Private treatment providers are in the midst of an unprecedented controversy surrounding ethics. There is ongoing debate about evidence-based treatment. Abstinence based organizations and medication assistance advocates each dig in and establish their righteous positions.
Status quo organizations do not want new programs and new approaches to come on board.
The recovery movement has its own ethical controversies. Pharmaceutical companies are a player, whether we want to admit it or not. There are new advocacy organizations popping up every other day.
Public treatment providers have a lobbyist group that ensures public funding continues to funnel through the Single State Authority.
There are competing interests. Despite the fact most players consistently state there is “no competition”.
These complex and competing interests make innovation very difficult.
If we are going to innovate we are going to need to minimize push back. The effective innovator will need to understand “both sides of the fence” and nurture relationships across these competing domains.
THE FUNDING –
HBR states
“Innovation in health care presents two kinds of financial challenges: funding the innovation’s development and figuring out who will pay how much for the product or service it yields”.
Of course, this is a major barrier to innovation in addiction treatment and recovery services. Insurance companies and government policy makers have defined a relatively narrow scope of “reimbursable” services.
These reimbursement policies drive program development. Providers develop interventions, programs, and solutions. All based on “how they get paid”, rather than, “what’s best for the patient”. Who can blame them?
At its most fundamental level our “fee for service” model “incentivizes” multiple trips to treatment. Rinse and repeat is desirable from a business model standpoint.
A move toward value-based healthcare and reimbursement based on outcomes could go far in promoting true innovation. If we incentivize outcomes over episodes of care we may see new ideas emerge.
THE POLICY –
HBR states:
“Government regulation of health care can sometimes aid innovation (“orphan drug” laws provide incentives to companies that develop treatments for rare diseases) and sometimes hinder it (recent legislation in the United States placed a moratorium on the opening of new specialty hospitals that focus on certain surgical procedures). Thus, it is important for innovators to understand the extensive network of regulations that may affect a particular innovation and how and by whom those rules are enacted, modified, and applied”.
In the addiction treatment and recovery services domain regulation slows innovative and non-traditional services have difficulty in being recognized as legitimate alternatives. These restrictions are frequently tied to funding.
For example, only certain licensed professionals can provide reimbursable services. Recovery coaching services are rarely reimbursed. Services can only be delivered in “licensed clinics”.
The program is restricted to working with the “identified patient”.
These regulations ensure most providers stay within the box. Otherwise you go out of business.
The key is to find alternative funding to implement the innovation. This will give the innovator a chance to demonstrate the effectiveness and value of the innovation which could lead to eventual regulatory approval. This could ultimately lead to reimbursement.
What do we do?
The first step is always awareness and recognition. If we consider ourselves innovators we must recognize these challenges and game-plan accordingly. There is nothing easy about innovation.
We will need to work with all of players to challenge the existing funding and regulations.
But more important than anything.
We will need to come up with the innovative solutions required to meet the needs of 22 million untouched individuals with substance use disorder and 100 million plus overwhelmed family members.
I am a human being who dealt with a health condition called substance use disorder via a recovery program and lifestyle management strategies. For me it includes meetings, one to one support and continuous effort at self-improvement. I am forever grateful for those who helped me early.
However, it’s important to note: some of my greatest support has come from outside of the “Recovery Bubble”.
NOTE: **There was a time in the not so distant past where I would not say these type of things for fear I would get thrown out of the Recovery Club. Thankfully I’ve matured.**
I’m not some alien from another planet fundamentally different from all the other inhabitants of earth.
I reject the “normies” vs those in the recovery paradigm. I reject the addictive thinking paradigm. It’s “human thinking” not addictive thinking. I reject that I am not able to experience the full range of human emotions for fear that I may “pick up”. Anger is not to be feared.
I reject that I need to spend the rest of my life separating myself from humanity. I reject the paradigm that one must do recovery in a certain manner via a certain type of program.
I’m just a dude who doesn’t drink or use drugs. And I am interested in living life to the fullest. I have overcome a very serious healthcare issue and want to help others do the same. That’s it…. Period!
The Recovery Echo Chamber
Furthermore, I believe everyone is recovering from something. And rather than separating ourselves we should join together. It’s wellness. Health. Mental health. Emotional health. Only then will we impact society. Until then we will just continue to preach to the choir. Attending rallies full of other addictive thinking aliens.
SCREAMING AT THE TOP OF OUR LUNGS IN OUR ADDICTION RECOVERY ECHO CHAMBER.
I first noticed the universal nature of recovery when working with families. Many people promote a separation between the individual and the family. In general, the individual is encouraged to do their own recovery and the family may or may not engage.
Either way, the recovering individual enters into a secret society. However, as I began to work with families I saw undeniable similarities. For example:
The family also engaged in a behavior that, at first, provided a sense of relief. However, the behavior quickly turns into a self-destructive act that is compulsive in nature. For example, the family “uses” rescuing over and over despite clear consequences.
As time progresses, the family entered into a type of denial around both the seriousness of their loved one’s issues and the reality of their behaviors. This serves to protect the enabling behavior in the same way that denial helps the addicted individual protect his addiction.
I also saw that, just like the person in addiction, family members required support and intervention to get free from these cycles of self-destruction. Just like the addicted individual family members went through predictable stages of change.
Beyond the Bounds of Addiction
Then I began to look beyond substance use disorders. I am a certified EMDR trauma therapist and a Certified Employee Assistance Professional.
I own an EAP company and maintain a private practice. I see people who are dealing with a wide variety of issues. I have always known that recovery goes beyond the bounds of addiction.
However, I never thought much about it. Addiction was always the most significant issue and my obsession was eradicating it from my life and my kids lives. And…saving the world.
And then I began to reflect on my own life…
I selfishly moved my family to South Carolina for “my career” and turned their lives upside down.
I started to see my own daughter struggle through this isolative, fragmented, and disjointed world. A world made worse by my self-centered move and my tunnel vision surrounding addiction.
Her struggles weren’t related to addiction so I didn’t see them as I should have.
I had become so myopic in my views. I operated with the unspoken point of view that people grow out of toxic stress and emotional problems come and go. But addiction, that’s what we need to worry about. I tend to see the world through the lens of addiction. Everything goes back to addiction. (Hell, in today’s world everything goes back to the opioid epidemic and overdoses).
In the meantime, my daughter was navigating this ridiculous world of impression management, toxic masculinity, social media isolation, self-imposed pressure, and my absenteeism. She found herself associating with some of the most disingenuous fake people on the face of the planet.
I let her down. I did not defend her or support her as much as I should have because I was obsessed with saving the world from addiction. Fortunately, we have a strong family and she is a strong person. We have gotten control of this situation.
I’m sorry Elizabeth…. I won’t make this mistake again.
The Problems of this Society:
However, it makes me wonder. Why do we define recovery so narrowly and why do we ignore the enormity of the problems of this society:
We live in a world where 64% of college students report severe anxiety and panic attacks.
44,965 Americans die by suicide every year.
Suicide is the second leading cause of death for people age 10-24
Toxic masculinity is a real issue. It refers to the socially-constructed attitudes that describe the masculine gender role as violent, unemotional, sexually aggressive, and so forth.
Technology and social media has brought great progress. However, at the same time we are at its mercy.
Depression and loneliness is at an all time high. You can be constantly connected and constantly alone.
If you are marginalized in school or among your peers you are never going to be able to escape it due to the ever-present social media access. It’s like 24 hours 365 days of middle school.
It is for these reasons that the RECOVERY CARTEL will pivot just a bit.
We are going to maintain our focus on addiction. We intend to continue to bring you the most up to date and insightful information on recovery from addiction. However, we also intend to broaden our scope. We will focus on mental health, stress management, growing up, parenting, and all things recovery.
But please note: we intend to pursue these topics with the same vigor and aggression we bring to all things associated with the Recovery Cartel. We not going to go all “therapist” on you.
We believe that the most important aspect of recovery is human connection. Actually, we know that the most important aspect of recovery is human connection.
Addiction has been present among humans from the beginning.
There is no such a thing as Tough Love being effective or useful in combating addiction. References about addiction have been written about in the Bible:
“At last it (alcohol) bites like a serpent and stings like an adder. Your eyes will see strange things, and your mind utter perverse things (Proverbs 23:32-33)”.
The great philosopher, Plato was concerned about children under 18 drinking.
Over the course of history, society has struggled with how to approach this issue; and across the course of history people have been receiving absolutely ridiculous advice on how to handle addiction.
“For as long as there have been written records, people have been searching for what to do about the troublesome use of psychoactive drugs. Ancient Greek remedies for excessive alcohol use included placing an eel at the bottom of the unfortunate drinker’s generous goblet of red wine. Historically, problem drinkers have been whipped, dunked, shocked, poisoned with potions, chained, dialyzed, terrorized, and drugged with hallucinogens”.
Problematic and Ineffective
The war on drugs for example has been a war on people and completely ineffective.
Yet it remains our first line of defense and most well-funded response to this issue. We have been prescribed one size fits all services and everyday seems to bring more controversy and disagreement on the “solution”.
People with a substance use disorder are subject to the most outrageous of advice, and the instant experts are everywhere. Family members are also subject to this same type of misguided advice.
One could argue that the common direction given to family members is just as problematic as whipping, shocking or dialyzing an active addict.
Love Your Child to Death
This is most pronounced where parents are concerned. Parents are told they are “loving their child to death” and they frequently arrive to our programs beaten down and self-critical.
One of the most common introductions used by family members new to our group is: “My name is Mr. Jones and I am the poster child for enabling” followed by hanging of the head and body language that reflects a hopeless self-concept where parenting is concerned.
One of the most problematic things I have ever heard came from a person who described himself as a professional in the field. I had the unfortunate opportunity to witness him admonish a group of parents about “enabling” and instructed the entire group (with no real knowledge of the individual family situations) to detach, kick the kid out of the house, stop all contact with the person and “not even give him a baloney sandwich.
We could write an entire blog post on the sad reality of this person’s behavior.
Fortunately, this man may be an outlier (I hope) and most professionals or helpers would avoid going to that extreme.
However, one glance at the unethical, illegal and exploitative A&E television show Intervention will tell you the “kick the bum out” mentality still carries the day.
Guide by Clichés
Clichés tend to guide much of what happens in addiction treatment/recovery services.
There are several that have become universally accepted as guiding principles. Some of these clichés are useful and some are destructive.
“The most troublesome of these is the term Tough Love.”
It is most troubling because it is the most universally recognized of family recovery principles despite the fact it has been shown to be dangerous at worse; ineffective at best.
What Exactly is Tough Love?
We throw the term tough love around like it is the gospel truth.
However, do we have a generally agreed upon definition of Tough Love?
A simple search reveals the following definition:
• Tough love is an expression used when someone treats another person harshly or sternly with the intent to help them in the long run. … In most uses, there must be some actual love or feeling of affection behind the harsh or stern treatment to be defined as tough love. (Wikipedia)
• Love or affectionate concern expressed in a stern or unsentimental manner (as through discipline) especially to promote responsible behavior (Webster’s dictionary)
Harshly or Sternly
Pretty obvious right! The key terms and principles stand out clearly: “harshly or sternly”; “stern and unsentimental manner”; to promote responsible behavior over the long term.
Tough love sits comfortably under the umbrella of confrontation and punishment that guided the majority of the treatment and recovery programs over the past 40 years. Fortunately, that philosophy is being challenged.
But it is easy to see that tough love is part of that tradition. To get a better sense of tough love let’s look at the origins of this principle.
Where Did The Idea of “Tough Love” Come From?
As stated above the concept of tough love is rooted in the tradition of confrontation and punishment that has been such an integral part of addiction treatment and recovery services. Tough love has been the preferred advice given to family and friends as they struggle with a loved one’s addiction.
It made perfect sense given the default approach with addicts: confront, berate and belittle until they admit defeat.
At which point we can build them back up in a more acceptable manner. The tough love approach became mainstream as younger and younger people needed support.
It was a mainstay of the youth treatment movement (boarding schools, therapeutic schools, wilderness camps, behavioral camps etc…). Many kids were subject to these re-education efforts.
Many times, the treatment was horrific. Programs like “Straight Recovery” took tough love to an entirely new level. They are a great example of how good intentions can go horribly wrong.
Most of the time these abusive programs would claim anecdotal stories of “success” (not empirical) as justification for the misguided approach. Fortunately, there is an effort to clean up these abusive practices and much progress has been made where teen treatment is concerned.
Mother Jones Is Telling the Truth!
The online news media website Mother Jonesdescribes the origin of tough love and teens in the following manner: “This harsh approach to helping troubled teens has a long and disturbing history. No fewer than 50 teen programs… can trace their treatment philosophy, directly or indirectly, to an antidrug cult called Synanon.
Founded in 1958, Synanon sold itself as a cure for hardcore heroin addicts who could help each other by:
“breaking new initiates with isolation, humiliation, hard labor, and sleep deprivation”
The connection between Synanon and tough love is important. Synanon was notorious for its abusive practices. The people running Synanon were open about the philosophy.
We could spend a great deal of time exploring the psychological pathologies of the founder-Bill Dietrich-but for the time being it is important to focus on the tough love connection.
Treatment Model for Thousands
As the 1970’s progressed Synanon became the model for thousands of treatment programs across America. Although these programs were not as intense and abusive as Synanon, the culture of confrontation, punishment and belittling carried the day in many of these programs. It became the norm and tough love was launched into the mainstream.
Never Studied or Validated
Please NOTE: Like most other addiction treatment practices; tough love was never studied or validated as an effective approach. It was simply “declared effective” by the founders of these programs.
The other 2 factors that promulgated the universal acceptance of tough love:
1). The culture of the times and the psychological establishment’s pre-occupation with law and order and ensuring the maintenance of the proper middle-class family (post WW II mentality).
If the addict was an embarrassment and causing problems a punishing approach seemed most conducive to promoting “middle class decorum and material comfort”. Families wanted everything to look appropriate and polished. And tough love fits in well with that model.
2). The popular media thrives on confrontation and drama. Tough love provides that.
Being patient and using connection, family therapy and a measured/rational approach doesn’t play well in terms of ratings. A&E needs drama and confrontation to sell the show. They don’t want clinically sound interventions.
Unchallenged for 40 Years
When you put all of this together you get “tough love” as an unquestioned rule of thumb.
Tough love has remained unchallenged for 40 years. We are fortunate, however, to be living in this time. Today, tough love is being re-evaluated and looked at.
It has been found invalid and many new ideas are being put forward. Many will criticize this movement away from tough love as an “easier and softer way”. Well to that I say…thank you for the complement.
We Do Not Need Tough Love
We do not need TOUGH love. What we do need the appropriate expression of love.
In reality, however, we know that addiction is a family disease and impacts everyone. We also know that family and friends are more impactful than professionals; when it comes to changing outcomes related to addiction.
Therefore, it will be necessary for parents to change their behaviors.
As parents change their behaviors the child becomes more likely to change his behavior. But rather than tough love, think of it as the appropriate expression of love.
Love is an action word and setting limits and boundaries is part of the action of love.
Many times, saying no is an act of love. We can not just stand by and allow our child to self-destruct.
HOWEVER, we do not need to be “tough” while setting these boundaries.
We do not need to be “harsh” or “unsentimental” or “mean” when we set these boundaries. You do not need to completely detach and never talk your loved one. We can buy our kids lunch.
“We can certainly make them a baloney sandwich.”
Setting boundaries is the most important aspect of the process. Setting boundaries takes practice.